- Record: found
- Abstract: found
- Article: found
Progress Toward Polio Eradication — Worldwide, January 2018–March 2020
research-article
Anna N. Chard , PhD
1
,
2
,
,
S. Deblina Datta , MD
2 ,
Graham Tallis , MBBS
3 ,
Cara C. Burns , PhD
4 ,
Steven G.F. Wassilak , MD
2 ,
John F. Vertefeuille , PhD
2 ,
Michel Zaffran , MEng
3
26 June 2020
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
Since the Global Polio Eradication Initiative (GPEI) was established in 1988, two
of the three wild poliovirus (WPV) serotypes (types 2 and 3) have been eradicated.*
Transmission of WPV type 1 (WPV1) remains uninterrupted only in Afghanistan and Pakistan.
This report summarizes progress toward global polio eradication during January 1,
2018–March 31, 2020 and updates previous reports (
1
,
2
). In 2019, Afghanistan and Pakistan reported the highest number of WPV1 cases (176)
since 2014. During January 1–March 31, 2020 (as of June 19), 54 WPV1 cases were reported,
an approximate fourfold increase from 12 cases during the corresponding period in
2019. Paralytic poliomyelitis can also be caused by circulating vaccine-derived poliovirus
(cVDPV), which emerges when attenuated oral poliovirus vaccine (OPV) virus reverts
to neurovirulence following prolonged circulation in underimmunized populations (
3
). Since the global withdrawal of type 2-containing OPV (OPV2) in April 2016, cVDPV
type 2 (cVDPV2) outbreaks have increased in number and geographic extent (
4
). During January 2018–March 2020, 21 countries reported 547 cVDPV2 cases. Complicating
increased poliovirus transmission during 2020, the coronavirus disease 2019 (COVID-19)
pandemic and mitigation efforts have resulted in suspension of immunization activities
and disruptions to poliovirus surveillance. When the COVID-19 emergency subsides,
enhanced support will be needed to resume polio eradication field activities.
Poliovirus Vaccination
Since May 2016, after trivalent OPV (tOPV, containing types 1, 2, and 3 Sabin strains)
was withdrawn from use, only bivalent OPV (bOPV; containing types 1 and 3 Sabin strains)
and injectable inactivated poliovirus vaccine (IPV, containing antigens for all three
serotypes) have been used in routine immunization programs worldwide. In 2018,
†
estimated global coverage with at least 3 doses of poliovirus vaccine (Pol3) among
infants aged <1 year received through routine immunization services was 89%, and with
at least the recommended one full dose or two fractional doses of IPV (IPV1) was 72%.
Regional, national, and subnational coverage estimates varied widely. In 2018, estimated
national Pol3 coverage in Afghanistan was 73%, and IPV1 coverage was 66%; coverage
in Pakistan was 75% for both Pol3 and IPV1 (
5
).
In 2018, approximately 1.2 billion bOPV, 32 million IPV, and 16 million monovalent
OPV type 1 (mOPV1) doses were administered in 35 countries during 105 supplementary
immunization activities (SIAs)
§
supported by GPEI. In 2019, approximately 1 billion bOPV, 17 million IPV, and 36 million
mOPV1 doses were administered in 34 countries during 90 SIAs. Since the global withdrawal
of OPV2, the World Health Organization (WHO) Director-General must authorize release
of monovalent OPV type 2 (mOPV2) for use in countries experiencing cVDPV2 outbreaks;
in 2018, 100 million mOPV2 doses were used for outbreak response, 190 million in 2019,
and 60 million in 2020 to date.
Poliovirus Surveillance
WPV and cVDPV transmission is primarily detected by surveillance for acute flaccid
paralysis (AFP) among children aged <15 years and confirmed by stool specimen testing
in WHO-accredited laboratories within the Global Polio Laboratory Network. AFP surveillance
performance indicators
¶
for 40 countries during 2018–2019 have recently been reported (
6
). Among the 22 countries reporting WPV or cVDPV cases in 2018 and 2019, 11 (Afghanistan,
Benin, Burkina Faso, Burma [Myanmar],** Chad, Ethiopia, Ghana, Nigeria, Pakistan,
Somalia, and Zambia) met threshold criteria for the two main indicators for adequate
AFP surveillance nationally during both years; five countries (Central African Republic
[CAR], the Democratic Republic of the Congo [DRC], Malaysia, Papua New Guinea, and
the Philippines) did not meet criteria for adequate surveillance either year; and
five countries (Angola, Indonesia, Mozambique, Niger, and Togo) met criteria for both
surveillance indicators in 2018, but not in 2019. Indicators vary substantially at
subnational levels; national level indicators often obscure subnational underperformance
(
7
). Many countries with and without recent poliovirus transmission supplement AFP surveillance
with environmental surveillance (the testing of sewage for poliovirus), that allows
more rapid and sensitive detection of poliovirus circulation where implemented. Persistent
gaps in quality poliovirus surveillance are evident when genomic sequencing of isolates
identifies polioviruses after long periods of undetected circulation. Continued strengthening
of surveillance systems is necessary to confirm absence of poliovirus transmission.
Reported Poliovirus Cases and Isolations
Countries reporting WPV cases and isolations. No WPV cases have been identified outside
of Afghanistan, Nigeria, and Pakistan since 2015; the most recent reported onset of
a WPV1 case in Nigeria was in September 2016. In 2018, 33 WPV1 cases were reported
worldwide: 21 (64%) in Afghanistan and 12 (36%) in Pakistan (Figure) (Table 1).
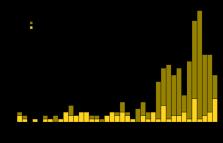
FIGURE
Number of cases of wild poliovirus, by country and month of onset — worldwide, January
2017–March 2020*
* Data are as of June 19, 2020.
The figure is a bar chart showing the number of cases of wild poliovirus, by country
and month of onset worldwide (Afghanistan 76; Pakistan 209) during January 2017–March
2020.
TABLE 1
Number of poliovirus cases, by country — worldwide, January 1, 2018–March 31, 2020*
Country
Reporting period
2018
2019
Jan–Mar 2019
Jan–Mar 2020
WPV1
cVDPV
WPV1
cVDPV
WPV1
cVDPV
WPV1
cVDPV
Countries with endemic WPV1 transmission
Afghanistan
21
0
29
0
6
0
12
2
Nigeria
0
34
0
18
0
8
0
1
Pakistan
12
0
147
22
6
0
42
44
Countries with reported cVDPV cases
Angola
0
0
0
130
0
0
0
2
Benin
0
0
0
8
0
0
0
1
Burkina Faso
0
0
0
1
0
0
0
4
Burma (Myanmar)†
0
0
0
6
0
0
0
0
Cameroon
0
0
0
0
0
0
0
3
Central African Republic
0
0
0
21
0
0
0
1
Chad
0
0
0
10
0
0
0
13
China
0
0
0
1
0
0
0
0
Côte d’Ivoire
0
0
0
0
0
0
0
5
Democratic Republic of the Congo
0
20
0
88
0
2
0
5
Ethiopia
0
0
0
13
0
0
0
14
Ghana
0
0
0
18
0
0
0
11
Indonesia
0
1
0
0
0
0
0
0
Malaysia
0
0
0
3
0
0
0
1
Mali
0
0
0
0
0
0
0
1
Mozambique
0
1
0
0
0
0
0
0
Niger
0
10
0
1
0
0
0
4
Papua New Guinea
0
26
0
0
0
0
0
0
Philippines
0
0
0
15
0
0
0
1
Somalia
0
12§
0
3
0
1
0
0
Togo
0
0
0
8
0
0
0
7
Zambia
0
0
0
2
0
0
0
0
Abbreviations: cVDPV = circulating vaccine derived poliovirus; WPV1 = wild poliovirus
type 1.
* Data are as of June 19, 2020.
† For this country, MMWR uses the U.S. State Department short-form name “Burma”; the
World Health Organization uses “Myanmar.”
§ One patient was coinfected with type 2 and type 3 cVDPV polioviruses.
Among 176 WPV1 cases reported during 2019, 29 (16%) were reported by Afghanistan,
representing a 38% increase over the 21 cases reported in 2018. Cases were reported
from 20 districts, a 43% increase from the 14 districts reporting cases during 2018.
Among 54 WPV1 cases detected during January–March 2020, 12 (22%) cases were detected
in 11 districts of 10 provinces in Afghanistan, compared with six cases reported in
six districts of three provinces during the same period in 2019. In Afghanistan, WPV1
was detected in 83 (25%) of 336 sewage samples collected from 15 of 20 (75%) sites
at regular intervals in 2018 and 56 (22%) of 259 samples from 12 of 21 (57%) sites
in 2019 (Table 2).
TABLE 2
Number of circulating wild polioviruses (WPV) and circulating vaccine derived polioviruses
(cVDPV) detected through environmental surveillance — worldwide, January 1, 2018–March
31, 2020*
Country
Jan 1–Dec 31, 2018
Jan 1–Dec 31, 2019
Jan 1–Mar 31, 2019
Jan 1–Mar 31, 2020
No. of samples
No. (%) of isolates
No. of samples
No. (%) of isolates
No. of samples
No. (%) of isolates
No. of samples
No. (%) of isolates
Countries with reported WPV1 cases (no. and % of isolates refer to WPV1)
Afghanistan
336
83 (25)
259
56 (22)
69
22 (32)
88
9 (14)
Pakistan
689
139 (20)
786
371 (47)
179
86 (47)
201
123 (61)
Countries with reported cVDPV cases† (cVDPV type) (no. and % of isolates refer to
cVDPVs)
Afghanistan (2)
336
0 (—)
259
0 (—)
69
0 (—)
88
17 (19)
Angola (2)
106
0 (—)
106
17 (16)
24
0 (—)
13
0 (—)
Benin (2)
0
—
37
0 (—)
0
—
15
0 (—)
Burkina Faso (2)
50
0 (—)
52
0 (—)
12
0 (—)
18
0 (—)
Burma (Myanmar)§ (1)
59
0 (—)
12
0 (—)
9
0 (—)
6
0 (—)
Cameroon (2)
684
0 (—)
602
4 (1)
130
0 (—)
65
1 (2)
Central African Republic (2)
128
0 (—)
149
9 (6)
28
0 (—)
24
2 (8)
Chad (2)
151
0 (—)
198
10 (5)
46
0 (—)
30
3 (10)
China (2)
171
1 (1)
201
0 (—)
49
0 (—)
51
0 (—)
Cote d’Ivoire (2)
173
0 (—)
154
7 (5)
42
0 (—)
48
24 (50)
Democratic Republic of the Congo (2)
189
1 (1)
294
0 (—)
61
0 (—)
45
0 (—)
Ethiopia (2)
81
0 (—)
140
2 (1)
38
0 (—)
15
0 (—)
Ghana (2)
33
0 (—)
202
17 (9)
46
0 (—)
52
16 (31)
Indonesia (1)
117
0 (—)
174
0 (—)
45
0 (—)
31
0 (—)
Malaysia (1, 2)
0
—
60
15 (25)
10
0 (—)
177
11 (6)
Mali (2)
51
0 (—)
48
0 (—)
12
0 (—)
12
0 (—)
Mozambique (2)
90
0 (—)
76
0 (—)
15
0 (—)
15
0 (—)
Niger (2)
221
0 (—)
293
0 (—)
66
0 (—)
59
0 (—)
Nigeria (2)
166
44 (27)
211
64 (30)
483
38 (8)
347
0 (—)
Pakistan (2)
689
0 (—)
786
39 (5)
179
0 (—)
201
13 (6)
Papua New Guinea (1)
17
7 (41)
75
0 (—)
23
0 (—)
0
—
Philippines (1, 2)
87
0 (—)
212
33 (16)
30
0 (—)
87
4 (5)
Somalia (2)
422
30 (7)
92
5 (5)
32
2 (6)
25
8 (32)
Togo (2)¶
0
—
0
—
0
—
0
—
Zambia (2)
130
0 (—)
256
0 (—)
65
0 (—)
14
0 (—)
Abbreviations: cVDPV = circulating vaccine derived poliovirus; WPV1 = wild poliovirus
type 1.
* Data are as of June 19, 2020.
† cVDPV2 was isolated from environmental samples in Kenya (2018) and in Malaysia (2019–2020),
but these isolations were not associated with cVDPV2 acute flaccid paralysis cases.
§ For this country, MMWR uses the U.S. State Department short-form name “Burma”; the
World Health Organization uses “Myanmar.”
¶ Country does not conduct environmental surveillance.
Pakistan reported 147 (84%) of the 176 WPV1 cases in 2019, an elevenfold increase
over the 12 cases reported in 2018; cases were reported in 43 districts, a sixfold
increase over the six districts with confirmed cases in 2018. During January–March
2020, 42 (78%) WPV1 cases were detected in four provinces (Balochistan, Khyber Pakhtunkhwa,
Punjab, and Sindh), a sixfold increase over the six cases in three provinces (Khyber
Pakhtunkhwa, Punjab, and Sindh) reported during the corresponding period in 2019.
In Pakistan, WPV1 was detected in 139 (20%) of 689 environmental surveillance samples
from 37 of 58 (64%) sites in 2018 and 371 (47%) of 786 samples from 56 of 60 (93%)
sites in 2019 (Table 2). WPV1 of Pakistan origin was detected in three environmental
surveillance samples in Iran in early 2019.
Countries reporting cVDPV cases and isolations. During January 2018–March 2020, cVDPV
transmission was confirmed in 26 countries. Five countries (Burma [Myanmar], Indonesia,
Malaysia, Papua New Guinea, and the Philippines) reported four cVDPV type 1 emergences,
with isolates from 39 AFP cases and 40 environmental surveillance samples. Twenty-three
countries (Afghanistan, Angola, Benin, Burkina Faso, Cameroon, CAR, Chad, China, Côte
d’Ivoire, DRC, Ethiopia, Ghana, Kenya, Malaysia, Mali, Mozambique, Niger, Nigeria,
Pakistan, Philippines, Somalia, Togo, and Zambia) reported 49 cVDPV2 emergences, with
isolates from 547 AFP cases in 21 countries and 354 environmental surveillance samples
in 15 countries. Among these, the JIS-1 Nigeria emergence has spread to nine countries
(
3
,
4
,
6
). Emergence of cVDPV type 3 was detected in Somalia during 2018–2019, involving isolates
from seven AFP cases
††
and 11 environmental surveillance samples.
Discussion
WPV type 2 was certified as eradicated in 2015, and in October 2019, eradication of
indigenous WPV type 3, last detected in 2012, was certified. Nigeria, the only country
in the WHO African Region with indigenous WPV1 transmission after 2004, has had no
evidence of circulation since September 2016; immunization coverage and surveillance
in security-compromised northeast Nigeria have continued to improve. With no evidence
of any WPV transmission since September 2016, the African Region meets the 3-year
threshold without WPV detection required for certification and is eligible to be certified
polio-free in 2020.
§§
During January 2018–March 2020, however, transmission of both WPV1 and cVDPV2 markedly
increased. Despite 4 years (2014–2017) of declines in reported WPV1 cases in Afghanistan
and Pakistan, the high proportion of environmental surveillance samples with isolation
of WPV1 during that time indicated persistent transmission in the historic polio reservoirs.
Both countries face ongoing challenges, including vaccine refusals, polio campaign
fatigue, and reaching mobile populations (
8
,
9
). In Afghanistan, antigovernment elements banned house-to-house vaccination in most
southern and southeastern provinces during May–December 2018, then permitted vaccination
only at designated community sites during January–April 2019 (
9
). Vaccination campaigns were banned nationally from the end of April 2019 to the
end of September 2019. In Pakistan, the proportion of WPV1-positive sewage samples
increased in early 2018; the number of WPV1 cases began to rise in late 2018. In 2019,
the Pakistan polio program underwent a management review and is modifying its approach
to address longstanding community mistrust and vaccine hesitancy issues (
8
).
The frequency and geographic extent of cVDPV2 outbreaks also increased during the
reporting period, primarily because of the limited timeliness, quality, or scope of
mOPV2 outbreak response SIAs and the seeding of new emergences of cVDPV2 outside mOPV2
outbreak response areas. Since 2018, cVDPV2 outbreaks have affected three of six WHO
regions; most of the 23 affected countries are in Africa but also include Afghanistan
and Pakistan, where WPV1 is endemic. Preparations continue for use in late 2020 of
a genetically stabilized novel OPV2 (nOPV2), which has a substantially lower risk
of reversion to neurovirulence and seeding new VDPV2 emergences than does Sabin mOPV2
(
10
); nOPV2 will eventually replace mOPV2 in cVDPV2 outbreak response SIAs.
In March 2020, GPEI committed to using its extensive laboratory and surveillance network
and thousands of trained frontline polio workers to fully support country preparedness
and response to the global COVID-19 pandemic.
¶¶
To comply with global guidance on physical distancing during the COVID-19 pandemic,
WHO and other GPEI partners recommended postponing all outbreak response SIAs until
at least June 2020, and all preventive SIAs until the second half of 2020, with resumption
depending upon COVID-19 control status. Although routine immunization services have
been disrupted in most countries during the pandemic, GPEI is working to strengthen
immunization services for preventing outbreak-prone diseases, including poliomyelitis
and measles. GPEI has prioritized the continuation of AFP and environmental surveillance
activities to monitor the extent of poliovirus circulation during the coming months;
however, disruptions are occurring in the detection and investigation of AFP cases
and in the shipping and testing of stool and sewage samples. Despite these disruptions,
new areas of circulation have been identified, and preparations are underway to respond
in the near future.
To address the reasons for increased WPV1 transmission since 2018 and resume field
activities deferred because of response to COVID-19, it will be important for both
Afghanistan and Pakistan programs to revitalize community engagement to combat polio
campaign fatigue and vaccine hesitancy, strengthen the provision of basic health services,
and substantially improve the management and quality of immunization activities to
reach chronically missed children. In Afghanistan, continued negotiations with local
antigovernment elements to resume house-to-house vaccination campaigns is crucial
to reaching population immunity necessary to interrupt virus transmission. In Pakistan,
implementing the 2019 management review recommendations to improve program oversight,
managerial processes, and operational effectiveness is critical to strengthening SIA
implementation above performance to date in all WPV1 reservoirs; identifying and mitigating
the underlying challenges in underperforming districts is essential to ultimately
interrupt all WPV1 transmission. In addition, defining a broad strategy to more effectively
reach underserved minorities, including Pashtun populations, will be essential. Resuming
preventive and outbreak response SIAs that have been paused because of the COVID-19
pandemic is critical to ensuring continued progress toward polio eradication during
2020. In the interim, GPEI and affected countries are actively planning for the safe
resumption and scale-up of polio field activities when and where the COVID-19 emergency
allows.
Summary
What is already known about this topic?
Wild poliovirus type 1 (WPV1) transmission continues in Afghanistan and Pakistan.
Circulating vaccine-derived poliovirus (cVDPV) outbreaks occur in areas with low immunization
coverage.
What is added by this report?
Although WPV1 incidence declined annually during 2015–2017, cases in Afghanistan and
Pakistan have increased since 2018. The number and geographic spread of cVDPV type
2 (cVDPV2) outbreaks are increasing. The COVID-19 pandemic has resulted in suspension
of immunization activities and disruption of poliovirus surveillance.
What are the implications for public health practice?
Substantial efforts to address programmatic challenges are essential to safely restore
and scale-up polio field activities in 2020, including use of a stabilized type 2
oral poliovirus vaccine to prevent new cVDPV2 emergences.
Related collections
Most cited references7
- Record: found
- Abstract: found
- Article: found
Update on Vaccine-Derived Poliovirus Outbreaks — Worldwide, July 2019–February 2020
Mary Alleman, Jaume Jorba, Sharon A. Greene … (2020)

- Record: found
- Abstract: found
- Article: found
Progress Toward Polio Eradication — Worldwide, January 2017–March 2019
Sharon A. Greene, Jamal Ahmed, S Datta … (2019)

- Record: found
- Abstract: found
- Article: found
Progress Toward Polio Eradication — Worldwide, January 2016–March 2018
Farrah Khan, S Datta, Arshad Quddus … (2018)