- Record: found
- Abstract: found
- Article: found
Snake-like hypermobile masses in three chambers of the heart: very unusual metastasis of squamous cell carcinoma
case-report
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
Introduction
Metastatic disease of the heart is rare, with an incidence of 1.23% depending on the
autopsy series [1]. Metastasis can occur in various ways: through the lymph system,
direct extension, and hematogenous or intracavitary dissemination by direct extension
via the caval or pulmonary veins. Cardiac metastases mostly involve the pericardium
and with lower incidence the epicardium or the myocardium. However, only 5% of tumors
affect the endocardium [2]. Pericardial invasion usually occurs through lymphatic
propagation, while endocardial involvement mainly results from hematogenous dissemination
[2]. This rare form of metastasis leading to intracavitary, endocardial, or valvular
metastatic deposits mainly occurs in the right chambers and is only rarely seen in
the left chambers. This is attributed to the filtering role of the pulmonary circulation
and the slower flow in the right chambers [3].
We report a very rare case of squamous cell carcinoma-detected snake-like hypermobile
metastatic intracardiac masses in three chambers of the heart from an unknown primary
origin.
Case report
At 8 years after coronary artery bypass graft surgery a 53-year-old man was admitted
to the emergency room with sudden onset of dysarthria and left hemiparesis. His blood
pressure was 130/70 mm Hg, and the pulse was regular with no pulsus paradoxus. Cardiac
examination was normal except for a systolic ejection murmur. There was no marked
jugular venous distention or edema of the extremities. Radial and dorsal pedis arteries
were symmetrically palpable. Neurological examination revealed disturbance of consciousness,
dysarthria, and left hemiparesis. Electrocardiography was normal except for the rare
premature atrial contractions, and chest X-ray findings were in the normal ranges.
His erythrocyte sedimentation rate was high (56 mm/h), but other laboratory data were
in the normal ranges. Head magnetic resonance imaging (MRI) revealed multiple hyperintense
lesions on the bilateral cerebral hemisphere. A low-molecular-weight heparin, enoxaparin
was started. On the fourth day after he began to improve, gained his consciousness
and was able to talk again, recurrent transient ischemic attacks (TIA) began to occur,
causing transient loss of consciousness. For evaluation of the embolic source, we
performed transthoracic echocardiography. Two-dimensional echocardiography showed
highly mobile, snake-like structures with a slightly higher echodensity as compared
to myocardium, in the right and the left atria as well as the left ventricular apical
septum (Figure 1). There was moderate tricuspid valve regurgitation and minimal mitral
valve regurgitations. Wall motions and echo densities as well as the pericardium were
normal. Vena cava inferior was in normal calibration, and no mass was detected. A
primary cardiac tumor or probable metastasis was suspected. We were planning to perform
further diagnostic tests such as cardiac MRI, transesophageal echocardiography and
computed tomography scanning of the body; however, the patient experienced a severe
transient ischemic attack under anticoagulant therapy with a transient total loss
of consciousness and transient respiratory failure. The patient was referred to neurologists
and surgeons, and an urgent decision to operate was taken in order to prevent further
severe stroke. Thus, the diagnostic tests were delayed to the post-operative period
and surgery was planned to be done through the guidance of surgical exploration. An
open excision of the cardiac masses was performed (Figure 2).
Figure 1
Image depicting snake-like hypermobile masses (asterisk) in three chambers of the
heart (left atrium, right atrium and left ventricle)
Figure 2
Macroscopic view of the cardiac masses after surgical extraction was performed
In the surgical exploration report it was stated that when the pericardium was opened
there was not any gross pathology in the external surface of the heart. During the
cannulation of the superior vena cava, the cannula encountered an internal force.
The right atrium was thick with the palpation. The right atriotomy revealed a solid
mass infiltration of the inner surface of the right atrium, reaching 2 cm thickness
near the superior vena cava and 1 cm thickness near the inferior vena cava. There
were also separate, nearly 1 cm width solid infiltrative regions both on the interatrial
septum and near the aorta. After the resections of solid masses, the interatrial septum
was opened. In the left atrium, there was a solid mass attached to the interatrial
septum phenotypically similar to the ones in the right atrium. There was also a second
solitary mass between the left auricula and the mitral annulus. Their resections were
performed with part of the interatrial septum. The right ventricle was normal, but
the interventricular septum was thick. There was a solid, phenotypically similar mass
in the left ventricle tightly attached to the mid portion of the interventricular
septum and spreading to the cavity. The interventricular septum was thick and infiltrated.
The mass was resected with a small part of the septum, but further excessive resection
was not performed.
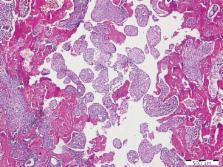
The histopathology of the surgical specimen revealed each mass to be a cardiac metastasis
of a highly differentiated squamous cell carcinoma from an unknown origin (Figure
3). Depending on the differentiation grade, the primary origin of the metastatic carcinoma
was thought to be from the nasopharyngeal region or lungs, but it is hard to define
the accurate region because of the lack of diagnostic tests. We also could not perform
further diagnostic tests as the patient's hemodynamic status was constantly unstable
in the post-operative period. In the post-operative period, low molecular weight heparin
infusion therapy and dual antiplatelet therapy with clopidogrel and acetylsalicylic
acid were continued as well as antibiotherapy with 1.5 g ampicillin/sulbactam 4 times
a day. However, the patient died due to renal failure and sepsis at eight days after
admission. After his death we did not obtain permission from the family members to
perform post mortem examinations on the body.
Figure 3
Histopathology of the surgical specimen revealed all three masses to be a cardiac
metastasis from an unknown origin of a squamous cell carcinoma
Discussion
We report a case with metastatic cardiac squamous cell carcinoma with an unknown primary
origin, presenting with stroke, involving the right atrium and both left heart chambers
simultaneously.
Cardiac metastases are far more common than are primary cardiac tumors. The reported
prevalence (1.5–20%) varies widely. They have a broad clinical presentation including
nonspecific symptoms, such as malaise, weight loss, chest pain, or congestive heart
failure secondary to intracardiac obstructions and valvular involvements, or pericardial
tamponade, arrhythmias or embolic events. Cardioembolic stroke accompanied with a
metastatic cardiac tumor, as in our case, seems to be quite rare; only several cases
have previously described [4].
Treatment options for patients with cardiac metastases are limited. They usually occur
in the context of disseminated carcinomatosis, which usually limits treatment to measures
aimed at relief of symptoms [5]. Due to the extent and location of the intracardiac
tumors, most patients were not also candidates for surgical resection. However, palliative
surgery may have a role in specific cases, such as obstruction of a cardiac chamber,
cardiac tamponade, symptoms arising from local progression of the tumor or high risk
of embolization. Prognosis is highly dependent on the stage and histological aggressiveness
of the tumor.
Echocardiography is the first-line imaging method to diagnose cardiac tumors as it
continues to be relatively inexpensive, readily available in most centers, repeatable,
and portable. This case illustrates the usefulness of early cardiac evaluation with
2-dimensional echocardiography in patients with stroke.
Finding the primary origin of such metastases and screening the whole body to assess
the extent of the disease have crucial importance for the management of patients.
Further diagnostic tests can be performed with magnetic resonance imaging, computed
tomography or transesophageal echocardiography for this purpose. In this particular
case unfortunately it was impossible to discover the primary origin of the metastatic
masses. We had some constraints limiting our further diagnostic work. Diagnostic tests
prior to surgery were lacking, as the urgent decision to operate was taken after the
consultation of the patient with neurologists and cardiovascular surgeons in order
to prevent further severe stroke. Unfortunately, the patient's hemodynamic status
did not let us perform any diagnostic tests in the post-operative period either. Moreover,
a post mortem examination could not be done because the family members did not give
the necessary legal permission.
Related collections
Most cited references4
- Record: found
- Abstract: found
- Article: not found
Cardiac tumours: diagnosis and management.
Jagdish Butany, Vidhya Nair, Ather Naseemuddin … (2005)
- Record: found
- Abstract: found
- Article: not found
Tumors of the heart. A 20-year experience with a review of 12,485 consecutive autopsies.
- Record: found
- Abstract: found
- Article: not found
The prognostic value of PET and PET/CT in cervical cancer
Perry W. Grigsby (2008)