- Record: found
- Abstract: found
- Article: found
Proposal of Two Prognostic Models for the Prediction of 10-Year Survival after Liver Resection for Colorectal Metastases
Read this article at
Abstract
Background
One-third of 5-year survivors after liver resection for colorectal liver metastases (CLM) develop recurrence or tumor-related death. Therefore 10-year survival appears more adequate in defining permanent cure. The aim of this study was to develop prognostic models for the prediction of 10-year survival after liver resection for colorectal liver metastases.
Methods
N=965 cases of liver resection for CLM were retrospectively analyzed using univariable and multivariable regression analyses. Receiver operating curve analyses were used to assess the sensitivity and specificity of developed prognostic models and their potential clinical usefulness.
Results
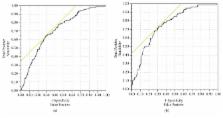
The 10-year survival rate was 15.2%. Age at liver resection, application of chemotherapies of the primary tumor, preoperative Quick's value, hemoglobin level, and grading of the primary colorectal tumor were independent significant predictors for 10-year patient survival. The generated formula to predict 10-year survival based on these preoperative factors displayed an area under the receiver operating curve (AUROC) of 0.716. In regard to perioperative variables, the distance of resection margins and performance of right segmental liver resection were additional independent predictors for 10-year survival. The logit link formula generated with pre- and perioperative variables showed an AUROC of 0.761.
Related collections
Most cited references27
- Record: found
- Abstract: found
- Article: not found
Phase III trial of infusional fluorouracil, leucovorin, oxaliplatin, and irinotecan (FOLFOXIRI) compared with infusional fluorouracil, leucovorin, and irinotecan (FOLFIRI) as first-line treatment for metastatic colorectal cancer: the Gruppo Oncologico Nord Ovest.
- Record: found
- Abstract: found
- Article: not found
Surgical resection of hepatic metastases from colorectal cancer: A systematic review of published studies
- Record: found
- Abstract: found
- Article: not found