- Record: found
- Abstract: found
- Article: found
Impact of previous sepsis on the accuracy of procalcitonin for the early diagnosis of blood stream infection in critically ill patients
Read this article at
Abstract
Background
Blood stream infections (BSI) are life-threatening infections in intensive care units (ICU), and prognosis is highly dependent on early detection. Procalcitonin levels have been shown to accurately and quickly distinguish between BSI and noninfectious inflammatory states in critically ill patients. It is, however, unknown to what extent a recent history of sepsis (namely, secondary sepsis) can affect diagnosis of BSI using PCT.
Methods
review of the medical records of every patient with BSI in whom PCT dosage at the onset of sepsis was available between 1 st September, 2006 and 31 st July, 2007.
Results
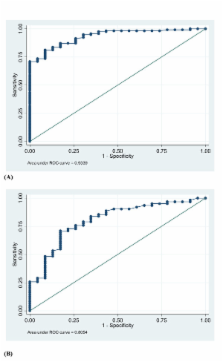
179 episodes of either primary ( n = 117) or secondary ( n = 62) sepsis were included. Procalcitonin levels were found to be markedly lower in patients with secondary sepsis than in those without (6.4 [9.5] vs. 55.6 [99.0] ng/mL, respectively; p < 0.001), whereas the SOFA score was similar in the two groups. Although patients in the former group were more likely to have received steroids and effective antibiotic therapy prior to the BSI episode, and despite a higher proportion of candidemia in this group, a low PCT value was found to be independently associated with secondary sepsis (Odd Ratio = 0.33, 95% Confidence Interval: 0.16–0.70; p = 0.004). Additional patients with suspected but unconfirmed sepsis were used as controls ( n = 23). Thus, diagnostic accuracy of PCT as assessed by the area under the receiver-operating characteristic curves (AUROCC) measurement was decreased in the patients with secondary sepsis compared to those without (AUROCC = 0.805, 95% CI: 0.699–0.879, vs. 0.934, 95% CI: 0.881–0.970, respectively; p < 0.050).
Related collections
Most cited references28
- Record: found
- Abstract: found
- Article: not found
Accuracy of procalcitonin for sepsis diagnosis in critically ill patients: systematic review and meta-analysis.
- Record: found
- Abstract: found
- Article: not found
Diagnostic value of procalcitonin, interleukin-6, and interleukin-8 in critically ill patients admitted with suspected sepsis.
- Record: found
- Abstract: found
- Article: not found
Procalcitonin as a diagnostic test for sepsis in critically ill adults and after surgery or trauma: a systematic review and meta-analysis.
Author and article information
Comments
Comment on this article
See how this article has been cited at scite.ai
scite shows how a scientific paper has been cited by providing the context of the citation, a classification describing whether it supports, mentions, or contrasts the cited claim, and a label indicating in which section the citation was made.