- Record: found
- Abstract: found
- Article: not found
Holistic management of DSD
Read this article at

Abstract
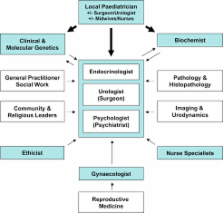
Disorder of sex development (DSD) presents a unique challenge, both diagnostically and in terms of acute and longer-term management. These are relatively rare conditions usually requiring a multidisciplinary approach from the outset and the involvement of a tertiary centre for assessment and management recommendations. This article describes the structure of the multidisciplinary team (MDT) at our centre, with contributions from key members of the team regarding their individual roles. The focus is on the newborn referred for assessment of ambiguous genitalia, rather than on individuals who present in the adolescent period or at other times, although the same MDT involvement is likely to be required. The approach to the initial assessment and management is discussed and the subsequent diagnosis and follow-up presented, with emphasis on the importance of careful transition and long-term support.
Related collections
Most cited references34
- Record: found
- Abstract: not found
- Article: not found
Consensus statement on management of intersex disorders.
- Record: found
- Abstract: found
- Article: not found
Matrix effects: the Achilles heel of quantitative high-performance liquid chromatography-electrospray-tandem mass spectrometry.
- Record: found
- Abstract: found
- Article: not found