- Record: found
- Abstract: found
- Article: found
Lichen sclerosus on the penis associated with striking elastic fibers accumulation (nevus elasticus) and differentiated penile intraepithelial neoplasia progressing to invasive squamous cell carcinoma
case-report
Denisa Kacerovska , MD, PhD
a
,
b ,
Michal Michal , MD
a
,
b ,
Milan Hora , MD, PhD
c ,
Ladislav Hadravsky , MD
a ,
Dmitry V. Kazakov , MD, PhD
a
,
b
,
∗
25 May 2015
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
Lichen sclerosus (LS) is a chronic disorder with a predilection for the anogenital
area. In this anatomic area, a subset of human papillomavirus–negative neoplasms arise
on the background of chronic inflammation, of which LS is the most common condition.
Of these neoplastic associations, squamous intraepithelial neoplasias, including the
differentiated (simplex) type of vulvar intraepithelial neoplasia and penile intraepithelial
neoplasia (PeIN), are salient lesions.
1
A rare and unusual feature in LS is a conspicuous accumulation of elastic fibers in
the level of the mid to lower part of the reticular dermis, sometimes strikingly apparent
on hematoxylin-eosin–stained slides. This condition was originally termed nevus elasticus,
2
but in a recent study the authors considered the process as hyperplastic.
3
To our knowledge, there are only 3 published clinicopathologic reports describing
this phenomenon.2, 3, 4 With respect to the anatomic site, all previously published
examples occurred on the vulva (with exception of 5 extragenital cases). We report,
a case of penile LS accompanied with conspicuous elastic fibers. Additionally, there
were areas of differentiated PeIN progressing into invasive squamous cell carcinoma.
Case report
A 70-year-old man presented with a flat, red-colored patch with irregular and poorly
defined margins on the glans penis. The surrounding skin showed a whitish hue (Fig
1). The lesion was asymptomatic and had been present for 5 years. A biopsy found features
of PeIN and invasive squamous cell carcinoma, and a simple glansectomy was performed.
The case is too recent for a meaningful clinical follow-up.
The removed tissue was fixed in 4% formaldehyde and embedded in paraffin. The paraffin
tissue blocks were cut into 5-μm-thick sections and stained with hematoxylin-eosin.
Histochemical staining for elastic fibers (Verhoeff-van Gieson, Elastic Stain [Sigma-Aldrich])
was performed. Immunohistochemical staining for p16 (clone E6H4, dilution RTU, Ventana,
Mannheim, Germany) and p53 (clone DO-7, dilution 1:400, Dako, Glostrup, Denmark) was
performed according to standard protocol.
Microscopically, both the initial biopsy specimens and the specimens from glansectomy
found histologic features of lichen sclerosus (ie, both a bandlike infiltrate composed
of predominantly lymphocytes and plasma cells with small foci of hemorrhage and sclerotic
collagen bundles with their homogenization in the superficial dermis). The epidermis
showed focally thinning; in other areas it was hyperplastic with atypical keratinocytes
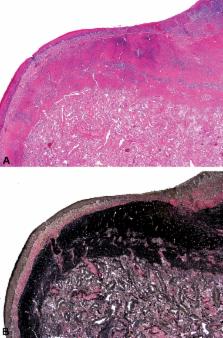
in the basal cell layer compatible with differentiated PeIN (Fig 2, A). In several
specimens, full-thickness atypia corresponding to carcinoma in situ was present and
foci of invasive squamous cell carcinoma were also revealed (Fig 2, B). The dysplastic
areas stained positively for p53 and were immunonegative for p16.
In the mid and reticular dermis there were striking areas of pink condensed finely
fibrillary and wavy material, which histochemically stained deeply for Verhoeff-van
Gieson and elastic stain confirming elastic etiology (Fig 3, A and B). This massive
increase in elastic fibers in the mid and lower part of reticular dermis contrasted
strikingly to their near absence in the superficial subepithelial tissues. Elastic
stains also found increased presence of elastic fibers around blood vessels in the
deeper portion of the dermis.
Discussion
Apart from collagen, an elastic fiber network is an important extracellular matrix
component extending throughout the dermis. In the normal skin, elastic fibers in the
reticular dermis are composed of a central core of amorphous, hydrophobic, cross-linked
elastin surrounded by connective tissue microfibrils, the principal structural component
of which is the glycoprotein fibrillin. In the papillary dermis, finer fibers containing
less elastin are found, which are termed elaunin fibers.
5
Although the precise nature of the alteration of an extracellular matrix in LS is
still poorly understood, Rahbari
6
in 1989 found a decrease in elastic fibers in LS.
The article reporting a strikingly increased number of elastic fibers in a case of
vulvar LS was published in 1990 by Sánchez Yus et al.
2
The authors interpreted this case as nevus elasticus and considered this unusual feature
to be unrelated to LS. Recently, a series of 18 cases of LS of the vulva and 4 cases
of extragenital LS associated with increased amount of elastic fibers in the mid to
lower part of the reticular dermis has been published.
3
In contrast to Sánchez Yus et al,
2
Shiba et al
3
suggested that this phenomenon is different from an authentic nevus elasticus and
may represent a repair process related to the loss of elastic fibers in the upper
part of the lesion. There is also on record a case of extragenital LS in a surgical
scar with an elastic fibers increase.
4
The most common elastic fiber alteration in the skin is solar elastosis caused by
chronic or longstanding sun exposure. Occasionally, areas of solar elastosis may be
sharply circumscribed with an apparent increase of collagen bundles resembling the
phenomenon discussed here. The very anatomic site, namely, the vulva and penis, however,
almost excludes the possibility of sun exposure to play a role in the pathogenesis
of the disease. Along this line, we are aware of cases of increased elastic fibers
in the vagina (A. Selim, personal communication, October 2013). A case of unusual
stromal elastosis associated with mammary-type tubulolobular carcinoma of the vulva
has been reported.
7
Elastic changes in that case were analogous to those seen in the mammary parenchyma
adjacent to a carcinoma.
In neither the original cases of Sánchez Yus et al
2
or in the series of Shiba et al
3
was there any case of epithelial dysplasia. Apart from the current case of differentiated
PeIN, we have in our files 4 cases of vulvar lesions displaying a combination of LS,
differentiated vulvar intraepithelial neoplasia, and increased elastic numbers. In
other words, all our cases of LS associated with strikingly increased elastic fibers
manifested dysplastic changes.
We describe a case of penile LS associated with conspicuous increase of elastic fibers
and epithelial dysplasia. The histologic picture is distinctive, with a sandwich-like
structure composed of the epithelium (normal or dysplastic), subepithelial homogenized
and sclerotic area, and sharply demarcated deeper elastosis. The mechanism of alterations
of elastic fibers is not currently known.
Related collections
Most cited references7
- Record: found
- Abstract: found
- Article: not found
Is differentiated vulval intraepithelial neoplasia the precursor lesion of human papillomavirus-negative vulval squamous cell carcinoma?
Fani Kokka, Naveena Singh, Asma Faruqi … (2011)
- Record: found
- Abstract: found
- Article: not found
Alterations in fibrillin as well as collagens I and III and elastin occur in vulval lichen sclerosus.
- Record: found
- Abstract: found
- Article: not found
Increase of elastic fibers in lichen sclerosus et atrophicus.
Yohei Shiba, Koji Ono, Minoru Akiyama … (2014)