- Record: found
- Abstract: found
- Article: found
Factors associated with inappropriate use of emergency departments: findings from a cross-sectional national study in France
Read this article at
Abstract
Background
Inappropriate visits to emergency departments (EDs) could represent from 20% to 40% of all visits. Inappropriate use is a burden on healthcare costs and increases the risk of ED overcrowding. The aim of this study was to explore socioeconomic and geographical determinants of inappropriate ED use in France.
Method
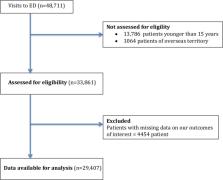
The French Emergency Survey was a nationwide cross-sectional survey conducted on June 11 2013, simultaneously in all EDs in France and covered characteristics of patients, EDs and counties. The survey included 48 711 patient questionnaires and 734 ED questionnaires. We focused on adult patients (≥15 years old). The appropriateness of the ED visit was assessed by three measures: caring physician appreciation of appropriateness (numeric scale), caring physician appreciation of whether or not the patient could have been managed by a general practitioner and ED resource utilisation. Descriptive statistics and multilevel logistic regression were used to examine determinants of inappropriate ED use, estimating adjusted ORs and 95% CIs.
Results
Among the 29 407 patients in our sample, depending on the measuring method, 13.5% to 27.4% ED visits were considered inappropriate. Regardless of the measure method used, likelihood of inappropriate use decreased with older age and distance from home to the ED >10 km. Not having a private supplementary health insurance, having universal supplementary health coverage and symptoms being several days old increased the likelihood of inappropriate use. Likelihood of inappropriate use was not associated with county medical density.
Conclusion
Inappropriate ED use appeared associated with socioeconomic vulnerability (such as not having supplementary health coverage or having universal coverage) but not with geographical characteristics. It makes us question the appropriateness of the concept of inappropriate ED use as it does not consider the distress experienced by the patient, and segments of society seem to have few other choices to access healthcare than the ED.
Related collections
Most cited references57
- Record: found
- Abstract: found
- Article: not found
Emergency department visits for nonurgent conditions: systematic literature review.
- Record: found
- Abstract: found
- Article: not found
Continuity of primary care and emergency department utilization among elderly people.
- Record: found
- Abstract: found
- Article: not found