- Record: found
- Abstract: found
- Article: found
Dialysis with high-flux membranes significantly affects plasma levels of neutrophil gelatinase-associated lipocalin
letter

Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
I read with interest the recent article by Schilder et al. reporting that plasma levels
and the biomarker value of neutrophil gelatinase-associated lipocalin (NGAL) in critically
ill patients with acute kidney injury (AKI) are not affected by continuous venovenous
hemofiltration (CVVH) [1]. Recently, Honore et al. [2] commented on the data by Schilder
et al., suggesting that further studies are warranted to definitely assess the membranes
and the dialytic techniques that can remove NGAL from plasma and thus affect its accuracy
as a marker of AKI.
Our results in 31 patients on maintenance hemodialysis (MHD), published in Critical
Care as part of a study that evaluated the effect of glomerular filtration rate impairment
on diagnostic performance of NGAL [3], appear quite different from those found by
Schilder et al. in critically ill patients who received CVVH. Patients on MHD received
low-flux dialysis (23 treatments) with a polysulfone membrane (F8; Fresenius, Bad
Homburg, Germany), or different high-flux membranes. High-flux dialysis treatments
were performed in 13 patients by using a triacetate cellulose membrane with a surface
of 1.9 m2 and an ultrafiltration rate (UFR) of 8474 mL/h per 100 mm Hg (N190 FH; Nipro,
Osaka, Japan). The remaining eight treatments were performed as hemodiafiltration
with a polyphenylene membrane with a surface of 2.0 m2 and a UFR of 6800 mL/h per
100 mm Hg (Phylther; Bellco, Mirandola, Italy) or as an acrylonitril and natrium metallylsulfone
copolymer membrane with a surface of 2.15 m2 and a UFR of 6500 mL/h per 100 mm Hg
(Nephral 500; Gambro, Lund, Sweden). Dialysis length was 4.0 ± 0.2 h, and blood flow
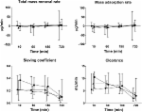
was 312 ± 43 mL/min. Mean plasma concentrations of NGAL increased by 9.1 ± 24.4 %
at the end of low-flux dialysis, indicating that low-flux polysulfone did not remove
NGAL (Fig. 1). Treatments with high-flux membranes decreased plasma NGAL significantly
(P < 0.0001). The reduction ratio of NGAL was higher after hemodiafiltration (52.1 ± 26.7 %)
than after high-flux dialysis (26.6 ± 26.1 %, P = 0.053).
Fig. 1
Effect of dialysis with low-flux (LF) or high-flux (HF) membranes on plasma concentrations
of neutrophil gelatinase-associated lipocalin (NGAL) in 31 patients on maintenance
hemodialysis
Schilder et al. performed CVVH treatments with a triacetate membrane with a surface
of 1.9 m2 (UF-205), a UFR of 3700 mL/h per 100 mm Hg lower than that of our triacetate
membrane, and a lower sieving coefficient for middle molecules (0.81 versus 0.91 for
myoglobin). During treatments, the blood flow was kept at 180 mL/min and the substitution
fluid at 2 L/h. These differences can justify, at least in part, the lower removal
of NGAL found in patients with AKI than in patients on MHD.
Besides the chemical composition of the membrane, different parameters of the dialysis
session may influence the removal of NGAL. Therefore, further studies are warranted
to assess the membranes and the dialytic techniques that can affect the accuracy of
NGAL as a marker of AKI.
Related collections
Most cited references3

- Record: found
- Abstract: found
- Article: found
The plasma level and biomarker value of neutrophil gelatinase-associated lipocalin in critically ill patients with acute kidney injury are not affected by continuous venovenous hemofiltration and anticoagulation applied
Louise Schilder, S Nurmohamed, Pieter M. ter Wee … (2014)
- Record: found
- Abstract: found
- Article: found
Is neutrophil gelatinase-associated lipocalin unaffected by convective continuous renal replacement therapy? Definitely … maybe
Patrick M. Honore, Rita Jacobs, Inne Hendrickx … (2015)