- Record: found
- Abstract: found
- Article: found
Diagnostic accuracy of clinical tools for assessment of acute stroke: a systematic review
Read this article at
Abstract
Introduction
Recanalisation therapy in acute ischaemic stroke is highly time-sensitive, and requires early identification of eligible patients to ensure better outcomes. Thus, a number of clinical assessment tools have been developed and this review examines their diagnostic capabilities.
Methods
Diagnostic performance of currently available clinical tools for identification of acute ischaemic and haemorrhagic strokes and stroke mimicking conditions was reviewed. A systematic search of the literature published in 2015–2018 was conducted using PubMed, EMBASE, Scopus and The Cochrane Library. Prehospital and in-hospital studies with a minimum sample size of 300 patients reporting diagnostic accuracy were selected.
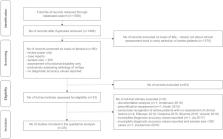
Results
Twenty-five articles were included. Cortical signs (gaze deviation, aphasia and neglect) were shown to be significant indicators of large vessel occlusion (LVO). Sensitivity values for selecting subjects with LVO ranged from 23 to 99% whereas specificity was 24 to 97%. Clinical tools, such as FAST-ED, NIHSS, and RACE incorporating cortical signs as well as motor dysfunction demonstrated the best diagnostic accuracy. Tools for identification of stroke mimics showed sensitivity varying from 44 to 91%, and specificity of 27 to 98% with the best diagnostic performance demonstrated by FABS (90% sensitivity, 91% specificity). Hypertension and younger age predicted intracerebral haemorrhage whereas history of atrial fibrillation and diabetes were associated with ischaemia. There was a variation in approach used to establish the definitive diagnosis. Blinding of the index test assessment was not specified in about 50% of included studies.
Conclusions
A wide range of clinical assessment tools for selecting subjects with acute stroke has been developed in recent years. Assessment of both cortical and motor function using RACE, FAST-ED and NIHSS showed the best diagnostic accuracy values for selecting subjects with LVO. There were limited data on clinical tools that can be used to differentiate between acute ischaemia and haemorrhage. Diagnostic accuracy appeared to be modest for distinguishing between acute stroke and stroke mimics with optimal diagnostic performance demonstrated by the FABS tool. Further prehospital research is required to improve the diagnostic utility of clinical assessments with possible application of a two-step clinical assessment or involvement of simple brain imaging, such as transcranial ultrasonography.
Related collections
Most cited references33
- Record: found
- Abstract: found
- Article: not found
Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke.
- Record: found
- Abstract: found
- Article: not found
Field Assessment Stroke Triage for Emergency Destination: A Simple and Accurate Prehospital Scale to Detect Large Vessel Occlusion Strokes.
- Record: found
- Abstract: found
- Article: not found