- Record: found
- Abstract: found
- Article: found
Predicting viral load suppression by self-reported adherence, pharmacy refill counts and real time medication monitoring among people living with HIV in Tanzania
Read this article at
Abstract
Introduction
Monitoring of adherence to antiretroviral treatment (ART) is of utmost importance to prevent treatment failure. Several measures to monitor adherence have been applied in low-resource settings and they all have pros and cons. Our objective was to examine whether any of the following adherence measures is a better predictor of participants’ viral load suppression: (1) self-report, (2) pharmacy refill count, (3) Real Time Medication Monitoring (RTMM), (4) a combination of self-report and pharmacy refill count or (5) all three adherence assessment methods combined.
Methodology
This was a post-hoc analysis of data from our 48-week REMIND-HIV randomized controlled trial in which adherence to ART was measured using self-report, pharmacy refill counts and RTMM among ART-experienced adults living with HIV subjectively judged to be nonadherent to ART. For each adherence measure, we calculated sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) for predicting virological failure defined as a viral load (VL) of > 20 copies/mL. To determine at which percentage of adherence the prediction was strongest, we evaluated adherence cut-offs of 80%, 85%, 90%, 95% and 100% using receiver operating characteristic (ROC) curves. VL data were obtained after 48 weeks of follow-up in the trial.
Results
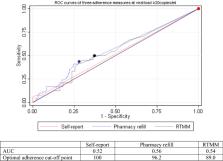
A total of 233 people living with HIV (PLHIV) were included in this analysis. When comparing the ability of self-reported adherence with pharmacy refill count and RTMM adherence to predict viral load > 20 copies/ml, self-reported adherence had the lowest sensitivity, ranging from 6 to 17%, but the highest specificity, ranging from 100 to 86%, depending on cut-off values from 80 to 100%. Area under the ROC curves (AUC) were 0.54 for RTMM, 0.56 for pharmacy refill count and 0.52 for self-report, indicating low discriminatory capacity for each of the adherence measures. When we combined the self-report and pharmacy refill count measures, sensitivity increased, ranging from 28 to 57% but specificity decreased, ranging from 83 to 53%. When all three measures were combined, we observed the highest value of sensitivity, ranging from 46 to 92%, and PPV, ranging from 32 to 36%, at high cut-offs ranging from 80 to 100%. Upon combination of three adherence measures, the AUC increased to 0.59.
Conclusion
Our results show that adherence assessed exclusively by self-report, pharmacy refill count or RTMM were insufficiently sensitive to predict virologic failure. Sensitivity markedly improved by combining all three measures, but the practical feasibility of such an approach would need to be studied.
Related collections
Most cited references40
- Record: found
- Abstract: found
- Article: not found
Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support.
- Record: found
- Abstract: found
- Article: not found
Adherence to protease inhibitor therapy and outcomes in patients with HIV infection.
- Record: found
- Abstract: found
- Article: not found