- Record: found
- Abstract: found
- Article: found
Prediction of Cardiovascular Events by Pulse Waveform Parameters: Analysis of CARTaGENE
Read this article at
Abstract
Background
Waveform parameters provide approximate data about aortic wave reflection. However, their association with cardiovascular events remains controversial and their role in cardiovascular prediction is unknown.
Methods and Results
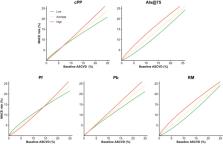
We analyzed participants aged between 40 and 69 from the population‐based CARTaGENE cohort. Baseline pulse wave analysis (central pulse pressure, augmentation index) and wave separation analysis (forward pressure, backward pressure, reflection magnitude) parameters were derived from radial artery tonometry. Associations between each parameter and major adverse atherosclerotic events (MACE; cardiovascular death, stroke, myocardial infarction) were obtained using adjusted Cox models. The incremental predictive value of each parameter compared with the 10‐year atherosclerotic cardiovascular disease score alone was assessed using hazard ratios, c‐index differences, continuous net reclassification indexes, and integrated discrimination indexes. From 17 561 eligible patients, 2315 patients had a MACE during a median follow‐up of 10.1 years. Central pulse pressure, forward pressure, and backward pressure, but not augmentation index and reflection magnitude, were significantly associated with MACE after full adjustment. All parameters except forward pressure statistically improved MACE prediction compared with the atherosclerotic cardiovascular disease score alone. The greatest prediction improvement was seen with augmentation index and reflection magnitude but remained small in magnitude. These 2 parameters enhanced predictive performance more strongly in patients with low baseline atherosclerotic cardiovascular disease scores. Up to 5.7% of individuals were reclassified into a different risk stratum by adding waveform parameters to atherosclerotic cardiovascular disease scores.
Related collections
Most cited references70
- Record: found
- Abstract: found
- Article: not found
A new equation to estimate glomerular filtration rate.

- Record: found
- Abstract: found
- Article: found
Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019
- Record: found
- Abstract: found
- Article: not found