- Record: found
- Abstract: found
- Article: found
The effect of intraoperative transnasal humidified rapid-insufflation ventilatory exchange on emergence from general anesthesia in patients undergoing microlaryngeal surgery: a randomized controlled trial

Read this article at
Abstract
Background
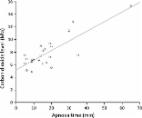
Transnasal humidified rapid-insufflation ventilatory exchange (THRIVE) has received extensive attention for its utility in tubeless anesthesia. Still, the effects of its carbon dioxide accumulation on emergence from anesthesia have not been reported. This randomized controlled trial aimed at exploring the impact of THRIVE combined with laryngeal mask (LM) on the quality of emergence in patients undergoing microlaryngeal surgery.
Methods
After research ethics board approval, 40 eligible patients receiving elective microlaryngeal vocal cord polypectomy were randomly allocated 1:1 to two groups, THRIVE + LM group: intraoperative apneic oxygenation using THRIVE followed by mechanical ventilation through a laryngeal mask in the post-anesthesia care unit (PACU), or MV + ETT group: mechanically ventilated through an endotracheal tube for both intraoperative and post-anesthesia periods. The primary outcome was duration of PACU stay. Other parameters reflecting quality of emergence and carbon dioxide accumulation were also recorded.
Results
Duration of PACU stay (22.4 ± 6.4 vs. 28.9 ± 8.8 min, p = 0.011) was shorter in the THRIVE + LM group. The incidence of cough (2/20, 10% vs. 19/20, 95%, P < 0.001) was significantly lower in the THRIVE + LM group. Peripheral arterial oxygen saturation and mean arterial pressure during intraoperative and PACU stay, Quality of Recovery Item 40 total score at one day after surgery and Voice Handicap Index-10 score at seven days after surgery were of no difference between two groups.
Related collections
Most cited references31
- Record: found
- Abstract: found
- Article: found
Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways
- Record: found
- Abstract: found
- Article: not found
Apnoeic oxygenation in adults under general anaesthesia using Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE) – a physiological study
- Record: found
- Abstract: found
- Article: not found