- Record: found
- Abstract: found
- Article: found
Vital Signs: Epidemiology and Recent Trends in Methicillin-Resistant and in Methicillin-Susceptible Staphylococcus aureus Bloodstream Infections — United States
Read this article at
Abstract
Introduction
Staphylococcus aureus is one of the most common pathogens in health care facilities and in the community, and can cause invasive infections, sepsis, and death. Despite progress in preventing methicillin-resistant S. aureus (MRSA) infections in health care settings, assessment of the problem in both health care and community settings is needed. Further, the epidemiology of methicillin-susceptible S. aureus (MSSA) infections is not well described at the national level.
Methods
Data from the Emerging Infections Program (EIP) MRSA population surveillance (2005–2016) and from the Premier and Cerner Electronic Health Record databases (2012–2017) were analyzed to describe trends in incidence of hospital-onset and community-onset MRSA and MSSA bloodstream infections and to estimate the overall incidence of S. aureus bloodstream infections in the United States and associated in-hospital mortality.
Results
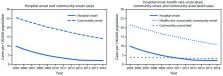
In 2017, an estimated 119,247 S. aureus bloodstream infections with 19,832 associated deaths occurred. During 2005–2012 rates of hospital-onset MRSA bloodstream infection decreased by 17.1% annually, but the decline slowed during 2013–2016. Community-onset MRSA declined less markedly (6.9% annually during 2005–2016), mostly related to declines in health care–associated infections. Hospital-onset MSSA has not significantly changed (p = 0.11), and community-onset MSSA infections have slightly increased (3.9% per year, p<0.0001) from 2012 to 2017.
Conclusions and Implications for Public Health Practice
Despite reductions in incidence of MRSA bloodstream infections since 2005, S. aureus infections account for significant morbidity and mortality in the United States. To reduce the incidence of these infections further, health care facilities should take steps to fully implement CDC recommendations for prevention of device- and procedure-associated infections and for interruption of transmission. New and novel prevention strategies are also needed.
Related collections
Most cited references18
- Record: found
- Abstract: found
- Article: not found
Invasive methicillin-resistant Staphylococcus aureus infections in the United States.
- Record: found
- Abstract: found
- Article: not found
Waves of resistance: Staphylococcus aureus in the antibiotic era.
- Record: found
- Abstract: found
- Article: not found