- Record: found
- Abstract: found
- Article: found
Prospective Case-Control Study of Cardiovascular Abnormalities 6 Months Following Mild COVID-19 in Healthcare Workers
Abstract
Objectives
The purpose of this study was to detect cardiovascular changes after mild severe acute respiratory syndrome coronavirus 2 infection.
Background
Concern exists that mild coronavirus disease 2019 may cause myocardial and vascular disease.
Methods
Participants were recruited from COVIDsortium, a 3-hospital prospective study of 731 health care workers who underwent first-wave weekly symptom, polymerase chain reaction, and serology assessment over 4 months, with seroconversion in 21.5% (n = 157). At 6 months post-infection, 74 seropositive and 75 age-, sex-, and ethnicity-matched seronegative control subjects were recruited for cardiovascular phenotyping (comprehensive phantom-calibrated cardiovascular magnetic resonance and blood biomarkers). Analysis was blinded, using objective artificial intelligence analytics where available.
Results
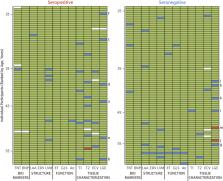
A total of 149 subjects (mean age 37 years, range 18 to 63 years, 58% women) were recruited. Seropositive infections had been mild with case definition, noncase definition, and asymptomatic disease in 45 (61%), 18 (24%), and 11 (15%), respectively, with 1 person hospitalized (for 2 days). Between seropositive and seronegative groups, there were no differences in cardiac structure (left ventricular volumes, mass, atrial area), function (ejection fraction, global longitudinal shortening, aortic distensibility), tissue characterization (T 1, T 2, extracellular volume fraction mapping, late gadolinium enhancement) or biomarkers (troponin, N-terminal pro–B-type natriuretic peptide). With abnormal defined by the 75 seronegatives (2 SDs from mean, e.g., ejection fraction <54%, septal T 1 >1,072 ms, septal T 2 >52.4 ms), individuals had abnormalities including reduced ejection fraction (n = 2, minimum 50%), T 1 elevation (n = 6), T 2 elevation (n = 9), late gadolinium enhancement (n = 13, median 1%, max 5% of myocardium), biomarker elevation (borderline troponin elevation in 4; all N-terminal pro–B-type natriuretic peptide normal). These were distributed equally between seropositive and seronegative individuals.
Central Illustration

Related collections
Most cited references39
- Record: found
- Abstract: found
- Article: not found
Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China
- Record: found
- Abstract: found
- Article: not found
An interactive web-based dashboard to track COVID-19 in real time

- Record: found
- Abstract: found
- Article: found
Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: prospective observational cohort study
Author and article information
Comments
Comment on this article
See how this article has been cited at scite.ai
scite shows how a scientific paper has been cited by providing the context of the citation, a classification describing whether it supports, mentions, or contrasts the cited claim, and a label indicating in which section the citation was made.