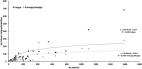
The novel SARS-CoV-2 (COVID-19) became a pandemic on 11 March 2020. The epidemiological picture is constantly evolving, and on 13 May, 4,170,424 cases and 287,399 confirmed deaths have been reported (WHO Report). People with COVID-19 infection may show several symptoms, including fever, cough, nausea, vomiting, dyspnea, myalgia, fatigue, arthralgia, headache, diarrhea, and rarely arthritis [1]. COVID-19 clinical features range from asymptomatic patients to acute respiratory distress syndrome (ARDS) and multiple organ dysfunction [2, 3]. Influenza symptoms are associated with a cascade of inflammatory mediators. Interleukin-6 (IL-6) and tumor necrosis factor-α (TNF- α) levels in plasma and upper respiratory secretions directly correlate with the magnitude of viral replication, fever, and respiratory and systemic symptoms, including musculoskeletal clinical manifestations [4, 5] Musculoskeletal symptoms such as fatigue, myalgia and arthralgia are common COVID-19 symptoms, but their prevalence has not yet been systematically investigated [6, 7]. We collected the published clinical data of the past 5 months to ascertain the prevalence of musculoskeletal symptoms and epidemiological characteristics published worldwide in COVID-19 patients. Data were tabulated using Microsoft ExcelTM 2020 V.16.34. The value was showed as mean ± SD. Student t test was used to reveal musculoskeletal symptoms between the total sample. To assess the incidence for each clinical variable, frequency analysis was performed. Regression analysis (R 2 ) was used to examine correlations between the total sample and musculoskeletal symptoms extracted. The level of significant was set at p < 0.05. The relevant reference and the data collected from the included articles are indicated in Tables 1 and 2. Table 1 Demographics Study (year) No. of patients Sex Age (mean SD or median IQR) Study design Country Zheng et al. [8] 99 M 51 F 48 49.40 (SD 18.45) Retrospective single center China Lei et al. [9] 34 M 14 F 20 55 (43–63) Retrospective single center China Mo et al. [10] 155 M 86 F 69 54 (42–66) Retrospective single center China Qian et al. [11] 91 M 37 F 54 50 (54–80) Retrospective multi-center China Ma et al. [12] 37 M 20 F 17 62 (59–70) Retrospective single center China Jin et al. [13] 651 M 331 F 246 46.0 (32–60) Retrospective multi-center China Zheng et al. [14] 161 M 80 F 81 45.0 (33.5–57) Retrospective single center China Wang et al. [15] 80 M 31 F 49 39.0 (32–48.5) Retrospective multi-center (electronic database) China Chen et al. [16] 203 M 108 F 95 54.0 (20–91) Retrospective single center China Zhou et al. [17] 21 M 13 F 8 66.1 (SD 13.94) Retrospective single center China Lo et al. [18] 10 M 3 F 7 54 (27–64) Retrospective single center China Huang et al. [19] 41 M 30 F 11 49.0 (41.0–58.0) Prospective multi-center (electronic database) China Zhang et al. [20] 645 M 328 F 317 46.65 (SD 13.82) Retrospective multi-center (electronic database) China Chen et al. [21] 249 M 126 F 123 51.0 (36–64) Retrospective single center China Feng et al. [22] 476 M 271 F 205 53.0 (40–64) Retrospective multi-center China Chen et al. [23] 274 M 171 F 103 62.0 (44–70) Retrospective single center China Zhang et al. [24] 140 M 71 F 69 57.0 (25–87) Retrospective multi-center China Lian et al. [25] 788 M 407 F 381 41.15 (SD 11.38) Retrospective multi-center (electronic database) China Cai et al. [26] 298 M 145 F 153 47.5 (33–61) Retrospective single center China Wan et al. [27] 135 M 72 F 63 47.0 (36–55) Retrospective single center China Cao et al. [28] 102 M 53 F 49 54.0 (37–67) Retrospective single center China Wang et al. [29] 339 M 166 F 173 69.0 (65–76) Retrospective single center China Xu et al. [30] 62 M 36 F 27 41.0 (32–52) Retrospective single center China Zhou et al. [31] 191 M 119 F 72 56.0 (46–67) Retrospective multi-center cohort study China Wu et al. [32] 201 M 128 F 73 51.0 (43–60) Retrospective single center cohort study China Du et al. [33] 85 M 62 F 23 65.8 Retrospective multi-center China Wang et al. [34] 69 M 32 F 37 42.0 (35–62) Retrospective single center China Guan et al. [35] 1099 M 640 F 459 47.0 (35–58) Retrospective multi-center China Goyal et al. [36] 393 M 238 F 155 62.2 (49–74) Retrospective multi-center USA Zhang et al. [37] 28 M 17 F 11 65.0 (56–70) Retrospective single center China Chen et al. [38] 118 M 0 F 118 31.0 (28–34) Retrospective single center China Wang et al. [39] 1012 M 524 F 488 50.0 (39–58) Retrospective multi-center China Xia et al. [40] 10 M 6 F 4 56.5 Retrospective single center China Liang et al. [41] 1590 M 904 F 674 48.9 (SD 16.3) Retrospective multi-center China Dai et al. [42] 234 M 136 F 98 44.6 Retrospective single center China Li et al. [43] 25 M 12 F 13 45.6 Retrospective single center China Chu et al. [44] 54 M 36 F 18 39 Retrospective single center China Qi et al. [45] 70 M 39 F 31 39.5 Retrospective multi-center China Godaert et al. [46] 17 M 8 F 9 86.5 Retrospective single center France Ye et al. [47] 5 M 2 F 3 30.0 Retrospective single center China Huang et al. [48] 22 M 6 F 16 22.0 (16.0–23.0) Retrospective single center China Tian et al. [49] 262 M 127 F 135 47.5 Retrospective single center China Huang et al. [50] 34 M 14 F 20 56.2 Retrospective single center China Xia et al. [51] 20 M 13 F 7 1.5 Retrospective single center China Zhao et al. [52] 101 M 56 F 45 44.44 Retrospective multi-center China Xu et al. [53] 51 M 25 F 26 41.6 Retrospective single center China Li et al. [54] 548 M 279 F 269 60.0 (48–69) Retrospective single center China Xu et al. [55] 90 M 39 F 51 50.0 (18–86) Retrospective single center China Lei et al. [56] 119 M 77 F 42 49.0 (SD 13.6) Retrospective multi-center China Pung et al. [57] 17 M 7 F 10 40.0 Retrospective single center Singapore Xu et al. [71] 50 M 29 F 21 42.3 Retrospective single center China Escalera-Antezana et al. [58] 12 M 6 F 6 36.5 Retrospective single center Bolivia Lechien et al. [59] 417 M 154 F 263 36.9 (SD 11.4) Retrospective multi-center Europe Dong et al. [72] 11 M 5 F 6 40.3 Retrospective single center China Total: 54 12.046 M 6427 (54%) F 5597 (46%) 52.13 Table 2 Musculoskeletal symptoms Study (year) No. of patients Fatigue (nr/%) Arthralgia/Myalgia (nr/%) Zheng et al. [37] 99 72 (73%) 12 (12%) Lei et al. [36] 34 25 (73.5%) 11 (32.4%) Mo et al. [60] 155 60 (73.2) 50 (61.0%) Qian et al. [61] 91 40 (43.96%) 5 (5.49%) Ma et al. [62] 37 4 (10.8%) 4 (10.8%) Jin et al. [10] 651 119 (18.2%) / Zheng et al. [11] 161 64 (39.8%) 18 (11.2%) Wang et al. [12] 80 28 (35%) 19 (23.75%) Chen et al. [13] 203 16 (7.9%) 54 (26.6) Zhou et al. [14] 21 5 (23.8%) 2 (9.5%) Lo et al. [15] 10 / 3 (30%) Huang et al. [16] 41 18 (44%) / Zhang et al. [17] 645 118 (18.3%) 71 (11%) Chen et al. [18] 249 39 (15.7%) / Feng et al. [19] 476 / 59 (12.4%) Chen et al. [20] 274 137 (50%) 60 (22%) Zhang et al. [58] 140 105 (75%) / Lian et al. [47] 788 139 (17.6%) 91 (11.5%) Cai et al. [21] 298 13 (4.3%) / Wan et al. [22] 135 / 44 (32.5%) Cao et al. [9] 102 56 (54.9%) 35 (34.3) Wang et al. [32] 339 135 (39.9%) 16 (4.7%) Xu et al. [26] 62 / 32 (52%) Zhou et al. [27] 191 44 (23%) 29 (15%) Wu et al. [29] 201 65 (32.3%) / Du et al. [33] 85 50 (58.8%) 14 (16.5%) Wang et al. [35] 69 29 (42%) 21 (30%) Guan et al. [33] 1099 419 (38%) 164 (15%) Goyal et al. [46] 393 / 94 (24%) Zhang et al. [24] 28 18 (64%) 4 (14%) Chen et al. [34] 118 19 (16%) / Wang et al. [41] 1012 / 170 (17%) Xia et al. [38] 10 3 (30%) / Liang et al. [39] 1590 680 (43%) 278 (17%) Dai et al. [40] 234 31 (13%) 21 (9%) Li et al. [41] 25 17 (68%) / Chu et al. [42] 54 9 (17%) 3 (6%) Qi et al. [43] 70 / 12 (17%) Godaert et al. [7] 17 10 (59%) / Ye et al. [28] 5 5 (100%) / Huang et al. [44] 22 5 (23%) 4 (18%) Tian et al. [45] 262 69 (26%) / Huang et al. [8] 34 / 22 (65%) Xia et al. [48] 20 1 (5%) / Zhao et al. [49] 101 / 17 (17%) Xu et al. [25] 51 2 (4%) 8 (16%) Li et al. [51] 548 258 (47%) 111 (20%) Xu et al. [52] 90 19 (21%) 25 (28%) Lei et al. [54] 119 / 18 (15%) Pung et al. [6] 17 / 5 (29%) Xu et al. [55] 50 8 (16%) 8 (16%) Escalera-Antezana et al. [59] 12 / 5 (42%) Lechien et al. [57] 417 129 (31%) 246 (59%) Dong et al. [56] 11 2 (18%) 1 (9%) Total: 54 Tot: 12,046 3085 (25.6%) 1866 (15.5%) Data on 12,046 patients (54% male and 46% females) were available. The number of patients in the selected studies ranged from 5 to 1590 patients (223 ± 312 patients). The sex ratio (male to female) was 1:15, and the overall average of patients was 52.13 years. The majority of the studies arose from China, mainly from Wuhan; one was from Singapore [57], two from Europe [46, 59], one from the USA [36], and one from Bolivia [58]. Musculoskeletal symptoms were present from the earliest stage of the viral illness and were reported in patients necessitating intensive care in the end stage of the condition. The total prevalence of fatigue symptom was 25.6% (R 2 =0.56; p value = 0.004), while the prevalence of arthralgia and/or myalgia was 15.5% (R 2 = 0.66; p value = 0.001; Fig. 1). Fig. 1 Relationships of fatigue and arthralgia/myalgia on all patients Eight studies reported a prevalence higher than 50% of patients with fatigue [8, 9, 24, 25, 28, 37, 46, 47], while three studies reported higher values for arthralgia/myalgia symptoms [50, 53, 59]. The prevalence of musculoskeletal symptoms in studies from Europe reached high values [46, 59]; Lechien et al., for example, reported on 417 COVID-19 patients from 12 European hospitals and found myalgia in 246 (59%) and arthralgia in 129 (31%) of these patients [59]. Clinical presentation of COVID-19 ranges from absence of symptoms to severe pneumonia. Fever, dry cough and fatigue are common symptoms, as indeed are myalgia and arthralgia [6, 53]. Most of the articles are retrospective single center studies: data were collected in a non-homogeneous way, especially regarding comorbidities, lifestyle habits, and severity of the illness. Based on our work, we cannot state, for example, whether children and younger patients less commonly present musculoskeletal symptoms at onset [63]. Most studies originate from China, which is not surprising, and it is not clear whether the prevalence of musculoskeletal symptoms at onset is influenced by socio-geographical factors [64]. The most common symptoms in patients with mild to moderate clinical presentation of the condition are fever, fatigue, and dry cough, followed by other symptoms including headache, nasal congestion, sore throat, myalgia, and arthralgia [65, 66]. The evidence on the central role of inflammation during COVID-19 infection underlines the need to block this inflammatory cascade [30, 60–62, 67–70]. The presence of musculoskeletal symptoms is worrying: there is a high rate of use, especially in the middle age and elderly population, of NSAIDs. The fact that patients therefore report musculoskeletal symptoms is even more worrying because it may imply that the inflammatory reactions overcome the anti-inflammatory effect of such drugs. Clinical features have to be analyzed deeply, especially considering the new evidences on COVID-19. Musculoskeletal symptoms should be married with laboratory findings, such as inflammatory and infection-related parameters (Interleukin-6, Procalcitonin, C-reactive protein). Understandably, the involvement of the musculoskeletal system has not been deeply investigated during this pandemic, but synovial and muscle biopsy, and joint fluid analysis, for example, should clarify how extensive the attack of the virus on the whole of the human body is. Until now, no report has been published on the presence of COVID-19 in the skeletal muscles, joint, or bones. The musculoskeletal symptoms are only anecdotally attributed to indirect effects, mainly arising from inflammatory and/or immune response, but other mechanisms can be hypothesized, such as direct damage by the virus on the endothelium or peripheral nerves. These findings could help to plan specific rehabilitation protocols in COVID-19 patients. As a new infectious disease, it is particularly important to underline the clinical features of COVID-19, especially in the early stage of the illness, to help clinicians to individuate and isolate patients earlier, and then minimize its diffusion. From the onset of the symptoms and to the most severe stages of COVID-19 disease, musculoskeletal symptoms, including myalgia, arthralgia, and fatigue, are a nearly constant presence. It is still unclear how the effects of COVID-19 on the musculoskeletal system are mediated.