- Record: found
- Abstract: found
- Article: found
Time to Regain Birthweight and Association with Neurodevelopmental Outcomes among Extremely Preterm Newborns
Read this article at
Abstract
Objective
Determine association between time to regain birthweight and 2-year neurodevelopment among extremely preterm (EP) newborns.
Study Design:
Secondary analysis of the Preterm Erythropoietin Neuroprotection Trial evaluating time to regain birthweight, time from birth to weight nadir, time from nadir to regain birthweight, and cumulative weight loss with 2-year corrected Bayley Scales of Infant and Toddler Development 3rd edition.
Results
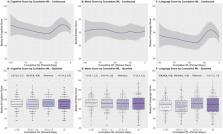
Among n = 654 EP neonates, those with shorter nadir-to-regain had lower cognitive scores (2–4 days versus ≥ 8 days: −3.5, [CI −7.0, 0.0]; ≤1 day versus ≥ 8 days: −5.0, [CI −10.2, 0.0]) in fully adjusted stepwise forward regression modeling. Increasingly cumulative weight loss was associated with lower cognitive scores (−50 to <−23 percent-days: −4.0, [95% CI −7.6, −0.4]) and language scores (≤−50 percent-days: −5.7, [CI −9.8, −1.6]; −50 to <−23 percent-days: −6.1, [CI −10.2, −2.0]).
Conclusion
Faster nadir-to-regain and prolonged, severe weight loss are associated with adverse 2-year neurodevelopmental outcomes.
Trial registration
PENUT Trial Registration: NCT01378273. https://clinicaltrials.gov/ct2/show/NCT01378273
Related collections
Most cited references25
- Record: found
- Abstract: found
- Article: not found
Simulation study of confounder-selection strategies.
- Record: found
- Abstract: found
- Article: not found
Growth in the neonatal intensive care unit influences neurodevelopmental and growth outcomes of extremely low birth weight infants.
- Record: found
- Abstract: found
- Article: not found