- Record: found
- Abstract: found
- Article: found
Morphological Analysis of the Sylvian Fissure Stem to Guide a Safe Trans-sylvian Fissure Approach
Read this article at
Abstract
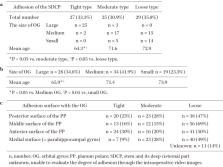
The sylvian fissure stem and its deep cisternal part (SDCP) consist mainly of the orbital gyrus (OG) and anterior medial portion of the temporal lobe. SDCP's adhesion has been found to make a trans-sylvian approach difficult due to the various patterns of adhesion. Thus, in this study, we aim to clarify the morphological features of the SDCP, and to guide a safe trans-sylvian approach. We retrospectively classified the morphology of the SDCP in 81 patients into 3 types (tight, moderate, loose type) according to the degree of adhesion of the arachnoid membrane and analyzed the morphological features of the OG and the temporal lobe using intraoperative video images. In addition, we have retrospectively measured each width of the SDCP's subarachnoid space at the three points (Point A, lateral superior portion; Point B, downward portion; Point C, medial inferior portion of SDCP) and analyzed their relationship to the degree of adhesion using the preoperative coronal three-dimensional computed tomography angiography (3D-CTA) images of 44 patients. As per the results, SDCP's adhesions were determined to be significantly tighter in cases with large OG and young cases. The temporal lobe had four surfaces (posterior, middle, anterior, and medial) that adhered to the OG in various patterns. The tighter the adhesion between the OG and each of the three distal surfaces of the temporal lobe, the narrower the width of the subarachnoid space at each point (A, B, C). Understanding of the morphological features of the SDCP, and estimating its adhesion preoperatively are useful in developing a surgical strategy and obtaining correct intraoperative orientation in the trans-sylvian approach.
Related collections
Most cited references37
- Record: found
- Abstract: found
- Article: not found
Microsurgical anatomy of the middle cerebral artery.
- Record: found
- Abstract: found
- Article: not found
Topographic anatomy of the insular region.
- Record: found
- Abstract: found
- Article: not found