There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
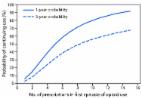
Because long-term opioid use often begins with treatment of acute pain ( 1 ), in March 2016, the CDC Guideline for Prescribing Opioids for Chronic Pain included recommendations for the duration of opioid therapy for acute pain and the type of opioid to select when therapy is initiated ( 2 ). However, data quantifying the transition from acute to chronic opioid use are lacking. Patient records from the IMS Lifelink+ database were analyzed to characterize the first episode of opioid use among commercially insured, opioid-naïve, cancer-free adults and quantify the increase in probability of long-term use of opioids with each additional day supplied, day of therapy, or incremental increase in cumulative dose. The largest increments in probability of continued use were observed after the fifth and thirty-first days on therapy; the second prescription; 700 morphine milligram equivalents cumulative dose; and first prescriptions with 10- and 30-day supplies. By providing quantitative evidence on risk for long-term use based on initial prescribing characteristics, these findings might inform opioid prescribing practices. A random 10% sample of patient records during 2006–2015 was drawn from the IMS Lifelink+ database, which includes commercial health plan information from a large number of managed care plans and is representative of the U.S. commercially insured population ( 3 ). The data are provided in a deidentified format and the institutional review board at the authors’ institution deemed the study was not human subject research. Records were selected of patients aged ≥18 years who had at least one opioid prescription during June 1, 2006–September 1, 2015, and ≥6 months of continuous enrollment without an opioid prescription before their first opioid prescription. Patients excluded were those who had any cancer (other than nonmelanoma skin cancer) or a substance abuse disorder diagnosis in the 6 months preceding their first opioid prescription, or whose first prescription was for any buprenorphine formulation indicated for treatment of substance abuse. Patients were followed from the date of their first prescription until loss of enrollment, study end date, or discontinuation of opioids, which was defined as ≥180 days without opioid use. The duration of use and number of prescriptions and cumulative dose (expressed in morphine milligram equivalents*) for the first episode of opioid use (defined as continuous use of opioids with a gap of no greater than 30 days) were calculated. The number of days’ supply and average daily dose in morphine milligram equivalents for the first prescription were also calculated. The first opioid prescription was categorized into six mutually exclusive categories: long-acting; oxycodone short-acting; hydrocodone short-acting; other Schedule II short-acting; Schedule III–IV and nalbuphine; and tramadol. † The Kaplan-Meier statistic was used to estimate median time to discontinuation of opioid use; probability of continued opioid use at 1 year and 3 years for different treatment duration thresholds (daily for 1–40 days and weekly for 1–26 weeks); number of prescriptions (1–15); and cumulative dose of the first episode of opioid use (50–2000 morphine milligram equivalents). Similarly, the relationship between the number of days’ supply, choice of first opioid prescription, and probability of continued opioid use at 1 and 3 years was also examined. Sensitivity analyses were conducted by modifying the discontinuation definition from ≥180 opioid-free days to ≥90 opioid-free days, changing the allowable gap in the first episode of opioid use from 30 days to 7 days, and excluding patients whose average daily dose of the first prescription exceeded 90 morphine milligram equivalents. A total of 1,294,247 patients met the inclusion criteria, including 33,548 (2.6%) who continued opioid therapy for ≥1 year. Patients who continued opioid therapy for ≥1 year were more likely to be older, female, have a pain diagnosis before opioid initiation, initiated on higher doses of opioids, and publically or self-insured, compared with patients who discontinued opioid use in 64% of patients who continued opioid use beyond 1 year were still on tramadol, suggesting that tramadol might be prescribed intentionally for chronic pain management. A 2016 study in Oregon ( 7 ), which did not include tramadol (a predictor of long-term use according to current data), reported similar findings: opioid naïve patients aged 1 week of opioids or when authorizing a refill or a second opioid prescription because these actions approximately double the chances of use 1 year later. In addition, prescribers should discuss the long-term plan for pain management with patients for whom they are prescribing either Schedule II long-acting opioids or tramadol. Summary What is already known about this topic? Based on the CDC Guideline for Prescribing Opioids for Chronic Pain, literature supporting long-term opioid therapy for pain is limited; research suggests an increased risk for harms with long-term opioid use. Early opioid prescribing patterns for opioid-naïve patients have been found to be associated with the likelihood of long-term use. What is added by this report? In a representative sample of opioid naïve, cancer-free adults who received a prescription for opioid pain relievers, the likelihood of chronic opioid use increased with each additional day of medication supplied starting with the third day, with the sharpest increases in chronic opioid use observed after the fifth and thirty-first day on therapy, a second prescription or refill, 700 morphine milligram equivalents cumulative dose, and an initial 10- or 30-day supply. The highest probability of continued opioid use at 1 and 3 years was observed among patients who started on a long-acting opioid followed by patients who started on tramadol. What are the implications for public health practice? Awareness among prescribers, pharmacists, and persons managing pharmacy benefits that authorization of a second opioid prescription doubles the risk for opioid use 1 year later might deter overprescribing of opioids. Knowledge that the risks for chronic opioid use increase with each additional day supplied might help clinicians evaluate their initial opioid prescribing decisions and potentially reduce the risk for long-term opioid use. Discussions with patients about the long-term use of opioids to manage pain should occur early in the opioid prescribing process.
Physicians, policymakers, and researchers are increasingly focused on finding ways to decrease opioid use and overdose in the United States both of which have sharply increased over the past decade. While many efforts are focused on the management of chronic pain, the use of opioids in surgical patients presents a particularly challenging problem requiring clinicians to balance 2 competing interests: managing acute pain in the immediate postoperative period and minimizing the risks of persistent opioid use after the surgery. Finding ways to minimize this risk is particularly salient in light of a growing literature suggesting that postsurgical patients are at increased risk for chronic opioid use. The perioperative care team, including surgeons and anesthesiologists, is poised to develop clinical- and systems-based interventions aimed at providing pain relief in the immediate postoperative period while also reducing the risks of opioid use longer term. In this paper, we discuss the consequences of chronic opioid use after surgery and present an analysis of the extent to which surgery has been associated with chronic opioid use. We follow with a discussion of the risk factors that are associated with chronic opioid use after surgery and proceed with an analysis of the extent to which opioid-sparing perioperative interventions (eg, nerve blockade) have been shown to reduce the risk of chronic opioid use after surgery. We then conclude with a discussion of future research directions.
scite shows how a scientific paper has been cited by providing the context of the citation, a classification describing whether it supports, mentions, or contrasts the cited claim, and a label indicating in which section the citation was made.