- Record: found
- Abstract: found
- Article: found
Cost-effectiveness analysis of cemiplimab vs pembrolizumab for treatment of advanced cutaneous squamous cell carcinoma
Read this article at
Abstract
BACKGROUND:
Most cutaneous squamous cell carcinomas (CSCCs) can be treated with surgical excision or radiation; however, approximately 1% of patients develop advanced disease. In 2018, the FDA approved cemiplimab-rwlc as the first programmed cell death-1 (PD-1) monoclonal antibody for the treatment of patients with metastatic CSCC or locally advanced CSCC who are not candidates for curative surgery or curative radiation. In June 2020, pembrolizumab, another PD-1 monoclonal antibody, was approved for the treatment of patients with recurrent or metastatic CSCC who are not candidates for curative surgery or radiation. We previously reported on the cost-effectiveness of cemiplimab vs historical standard of care for the treatment of advanced CSCC from a US perspective.
OBJECTIVE:
To estimate the cost-effectiveness of cemiplimab vs pembrolizumab for patients with advanced CSCC in the United States.
METHODS:
A “partitioned survival” framework was used to assess the cost-effectiveness of cemiplimab vs pembrolizumab. Clinical inputs were based on the most recent data cut of the phase 2 trials for cemiplimab (EMPOWER-CSCC-1; NCT02760498) and pembrolizumab (KEYNOTE-629). Progression-free survival and overall survival were extrapolated using parametric models until all patients had progressed or died. Health state utilities were derived from data collected in the EMPOWER-CSCC-1 trial. Costs included drug acquisition, drug administration, disease management, terminal care, and adverse events and were based on published 2020 US list prices. To assess model uncertainty, 1-way sensitivity and probabilistic sensitivity analyses (PSA) were conducted, alongside scenario analyses evaluating key modeling assumptions.
RESULTS:
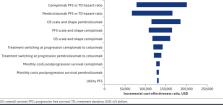
In the base case, cemiplimab resulted in an incremental gain of 3.44 life-years (discounted) and incremental cost-effectiveness ratio (ICER) of $130,329 per quality-adjusted life-year (QALY) vs pembrolizumab. At a willingness-to-pay threshold of $150,000/QALY, PSA indicated a 71% probability that cemiplimab is cost-effective when compared with pembrolizumab. Scenario analysis resulted in ICERs ranging from $115,909 to $187,374.
CONCLUSIONS:
Findings suggest that cemiplimab is a cost-effective treatment for patients with advanced CSCC, compared with pembrolizumab. These results should be interpreted cautiously in the absence of head-to-head trials; however, in the absence of such data, these results can be used to inform health care decisions over resource allocation.
Related collections
Most cited references51

- Record: found
- Abstract: found
- Article: found
The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials
- Record: found
- Abstract: not found
- Article: not found
Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement.
- Record: found
- Abstract: found
- Article: not found