- Record: found
- Abstract: found
- Article: found
Potential of trans fats policies to reduce socioeconomic inequalities in mortality from coronary heart disease in England: cost effectiveness modelling study
Read this article at
Abstract
Objectives To determine health and equity benefits and cost effectiveness of policies to reduce or eliminate trans fatty acids from processed foods, compared with consumption remaining at most recent levels in England.
Design Epidemiological modelling study.
Setting Data from National Diet and Nutrition Survey, Low Income Diet and Nutrition Survey, Office of National Statistics, and health economic data from other published studies
Participants Adults aged ≥25, stratified by fifths of socioeconomic circumstance.
Interventions Total ban on trans fatty acids in processed foods; improved labelling of trans fatty acids; bans on trans fatty acids in restaurants and takeaways.
Main outcome measures Deaths from coronary heart disease prevented or postponed; life years gained; quality adjusted life years gained. Policy costs to government and industry; policy savings from reductions in direct healthcare, informal care, and productivity loss.
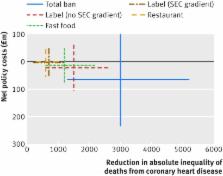
Results A total ban on trans fatty acids in processed foods might prevent or postpone about 7200 deaths (2.6%) from coronary heart disease from 2015-20 and reduce inequality in mortality from coronary heart disease by about 3000 deaths (15%). Policies to improve labelling or simply remove trans fatty acids from restaurants/fast food could save between 1800 (0.7%) and 3500 (1.3%) deaths from coronary heart disease and reduce inequalities by 600 (3%) to 1500 (7%) deaths, thus making them at best half as effective. A total ban would have the greatest net cost savings of about £265m (€361m, $415m) excluding reformulation costs, or £64m if substantial reformulation costs are incurred outside the normal cycle.
Conclusions A regulatory policy to eliminate trans fatty acids from processed foods in England would be the most effective and equitable policy option. Intermediate policies would also be beneficial. Simply continuing to rely on industry to voluntary reformulate products, however, could have negative health and economic outcomes.
Related collections
Most cited references33

- Record: found
- Abstract: found
- Article: found
Long Term Outcomes Following Hospital Admission for Sepsis Using Relative Survival Analysis: A Prospective Cohort Study of 1,092 Patients with 5 Year Follow Up

- Record: found
- Abstract: found
- Article: found
Preparation of Artificial Plasma Membrane Mimicking Vesicles with Lipid Asymmetry

- Record: found
- Abstract: found
- Article: found