- Record: found
- Abstract: found
- Article: found
The development of a lay health worker delivered collaborative community based intervention for people with schizophrenia in India
Read this article at
Abstract
Background
Care for schizophrenia in low and middle income countries is predominantly facility based and led by specialists, with limited use of non-pharmacological treatments. Although community based psychosocial interventions are emphasised, there is little evidence about their acceptability and feasibility. Furthermore, the shortage of skilled manpower is a major barrier to improving access to these interventions. Our study aimed to develop a lay health worker delivered community based intervention in three sites in India. This paper describes how the intervention was developed systematically, following the MRC framework for the development of complex interventions.
Methods
We reviewed the lierature on the burden of schizophrenia and the treatment gap in low and middle income countries and the evidence for community based treatments, and identified intervention components. We then evaluated the acceptability and feasibility of this package of care through formative case studies with individuals with schizophrenia and their primary caregivers and piloted its delivery with 30 families.
Results
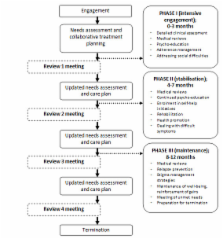
Based on the reviews, our intervention comprised five components (psycho-education; adherence management; rehabilitation; referral to community agencies; and health promotion) to be delivered by trained lay health workers supervised by specialists. The intervention underwent a number of changes as a result of formative and pilot work. While all the components were acceptable and most were feasible, experiences of stigma and discrimination were inadequately addressed; some participants feared that delivery of care at home would lead to illness disclosure; some participants and providers did not understand how the intervention related to usual care; some families were unwilling to participate; and there were delivery problems, for example, in meeting the targeted number of sessions. Participants found delivery by health workers acceptable, and expected them to have knowledge about the subject matter. Some had expectations regarding their demographic and personal characteristics, for example, preferring only females or those who are understanding/friendly. New components to address stigma were then added to the intervention, the collaborative nature of service provision was strengthened, a multi-level supervision system was developed, and delivery of components was made more flexible. Criteria were evolved for the selection and training of the health workers based on participants' expectations.
Related collections
Most cited references16
- Record: found
- Abstract: found
- Article: not found
Outcomes of people with psychotic disorders in a community-based rehabilitation programme in rural India
- Record: found
- Abstract: found
- Article: not found
Evaluation of a community-based rehabilitation model for chronic schizophrenia in rural India.
- Record: found
- Abstract: found
- Article: not found