- Record: found
- Abstract: found
- Article: not found
Pulmonary barotrauma in COVID-19: A systematic review and meta-analysis
Read this article at

Abstract
Background
An ever-increasing number of studies have reported an increased incidence of spontaneous pulmonary barotrauma such as pneumothorax, pneumomediastinum, and subcutaneous emphysema in patients with COVID-19. We conducted this systematic review and meta-analysis to assess the value and significance of the available data.
Methods
A thorough systematic search was conducted to identify studies of barotrauma in hospitalized patients with COVID-19. Data analysis of case reports was done using a statistical package for the social sciences (SPSS) version 22, and meta-analysis was performed using CMA-3.
Results
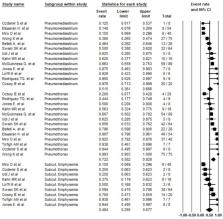
We identified a total of 4488 studies after thorough database searching.118 case reports and series, and 15 observational studies were included in the qualitative analysis. Fifteen studies were included in the quantitative analysis. The observational studies reported barotrauma in 4.2% (2.4–7.3%) among hospitalized patients; 15.6% (11–21.8%) among critically ill patients; and 18.4% (13–25.3%) in patients receiving invasive mechanical ventilation, showing a linear relationship of barotrauma with the severity of the disease. In addition, barotrauma was associated with a longer length of hospital stay, more extended ICU stay, and higher in-hospital mortality. Also, a slightly higher odds of barotrauma was seen in COVID-19 ARDS compared with non-COVID-19 ARDS.
Related collections
Most cited references33
- Record: found
- Abstract: found
- Article: found
AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both
- Record: found
- Abstract: found
- Article: not found
The PRISMA 2020 statement: An updated guideline for reporting systematic reviews
- Record: found
- Abstract: found
- Article: not found