- Record: found
- Abstract: found
- Article: found
Western Immunoblotting for the Diagnosis of Enterococcus faecalis and Streptococcus gallolyticus Infective Endocarditis
Read this article at
Abstract
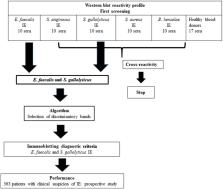
Blood culture-negative endocarditis (BCNE) remains a diagnostic challenge. In our center, despite a systematic and exhaustive microbiological diagnostics strategy, 22% of patients with BCNE remain without an identified etiology. In an effort to determine the relevance of using Western blot (WB) for the etiological diagnosis of BCNE in patients with early antibiotic use, we developed specific assays for the major infective endocarditis (IE) causative agents, namely, Staphylococcus aureus, Enterococcus faecalis, Streptococcus anginosus, and Streptococcus gallolyticus. Our technique was effective to identify the antigenic profiles of the four tested agents, but cross-reactions with S. aureus and S. anginosus antigens were frequent. A scoring method was developed for the diagnosis of E. faecalis and S. gallolyticus IE using the presence of reactivity to at least two antigenic bands for each bacterium and the positivity to at least one of the Ef300, Ef72, or Ef36 proteic bands for E. faecalis, and positivity for the two Sg75 and Sg97 proteic bands for S. gallolyticus. We tested these diagnostic criteria in a prospective cohort of 363 patients with suspected IE. Immunoblotting for the diagnosis of E. faecalis IE showed a sensitivity of 100% and a specificity of 99%. The positive and negative predictive values were 73 and 100%, respectively. Regarding S. gallolyticus infection, immunoblot had a sensitivity of 100% and a specificity of 95%. However, the positive predictive value was 22%, whereas the predictive negative value was 100%. Using WB, we identified a potential etiological agent in 4 of 14 BCNE cases with no identified pathogen. In conclusion, WB constitutes a promising and helpful method to diagnose E. faecalis or S. gallolyticus IE in patients with early antibiotic uptake and negative blood cultures.
Related collections
Most cited references9

- Record: found
- Abstract: found
- Article: not found
Serological cross-reactions between Bartonella and Chlamydia species: implications for diagnosis.
- Record: found
- Abstract: found
- Article: not found