- Record: found
- Abstract: found
- Article: found
Transnasal humidified rapid-insufflation ventilator exchange compared with laryngeal mask airway for endoscopic thoracic sympathectomy: a randomized controlled trial
Read this article at
Abstract
Background
Transnasal humidified rapid-insufflation ventilator exchange (THRIVE) has the characteristics of operating easily and maintaining oxygenation and eliminating CO 2, which makes it possible to be used in endoscopic thoracic sympathectomy (ETS). The application of THRIVE in ETS remains undefined. The purpose of this randomized controlled study is to assess the efficacy between THRIVE and laryngeal mask airway (LMA) for ETS.
Methods
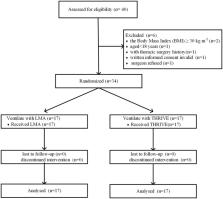
In total, 34 patients from May 2022 to May 2023 in Huazhong University of Science and Technology Union Shenzhen Hospital undergoing ETS were randomly divided into a THRIVE group ( n = 17) and an LMA group ( n = 17). A serial arterial blood gas analysis was conducted during the perioperative period. The primary outcome was the arterial partial pressure of carbon dioxide (PaCO 2) during the perioperative period. The secondary outcome was arterial partial pressure of oxygen (PaO 2) during the perioperative period.
Results
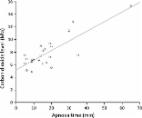
The mean (SD) highest PaCO 2 in the THRIVE group and LMA group were 99.0 (9.0) mmHg and 51.7 (5.2) mmHg, respectively ( p < 0.001). The median (inter-quartile range) time to PaCO 2 ≥ 60 mmHg in the THRIVE group was 26.0 min (23.2–28.8). The mean (SD) PaO 2 was 268.8 (89.0) mmHg in the THRIVE group and 209.8 (55.8) mmHg in the LMA group during surgery ( p = 0.027).
Related collections
Most cited references27
- Record: found
- Abstract: found
- Article: found
Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways
- Record: found
- Abstract: found
- Article: not found
Apnoeic oxygenation in adults under general anaesthesia using Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE) – a physiological study
- Record: found
- Abstract: found
- Article: not found