- Record: found
- Abstract: found
- Article: found
Plasma neutrophil gelatinase-associated lipocalin predicts acute kidney injury, morbidity and mortality after pediatric cardiac surgery: a prospective uncontrolled cohort study
Read this article at
Abstract
Introduction
Acute kidney injury (AKI) is a frequent complication of cardiopulmonary bypass (CPB). The lack of early biomarkers has impaired our ability to intervene in a timely manner. We previously showed in a small cohort of patients that plasma neutrophil gelatinase-associated lipocalin (NGAL), measured using a research enzyme-linked immunosorbent assay, is an early predictive biomarker of AKI after CPB. In this study we tested whether a point-of-care NGAL device can predict AKI after CPB in a larger cohort.
Methods
First, in a cross-sectional pilot study including 40 plasma samples (NGAL range 60 to 730 ng/ml) and 12 calibration standards (NGAL range 0 to 1,925 ng/ml), NGAL measurements by enzyme-linked immunosorbent assay and by Triage ® NGAL Device (Biosite Inc., San Diego, CA, USA) were highly correlated ( r = 0.94). Second, in a subsequent prospective uncontrolled cohort study, 120 children undergoing CPB were enrolled. Plasma was collected at baseline and at frequent intervals for 24 hours after CPB, and analyzed for NGAL using the Triage ® NGAL device. The primary outcome was AKI, which was defined as a 50% or greater increase in serum creatinine.
Results
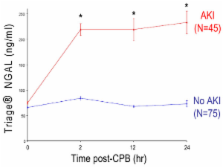
AKI developed in 45 patients (37%), but the diagnosis using serum creatinine was delayed by 2 to 3 days after CPB. In contrast, mean plasma NGAL levels increased threefold within 2 hours of CPB and remained significantly elevated for the duration of the study. By multivariate analysis, plasma NGAL at 2 hours after CPB was the most powerful independent predictor of AKI (β = 0.004, P < 0.0001). For the 2-hour plasma NGAL measurement, the area under the curve was 0.96, sensitivity was 0.84, and specificity was 0.94 for prediction of AKI using a cut-off value of 150 ng/ml. The 2 hour postoperative plasma NGAL levels strongly correlated with change in creatinine ( r = 0.46, P < 0.001), duration of AKI ( r = 0.57, P < 0.001), and length of hospital stay ( r = 0.44, P < 0.001). The 12-hour plasma NGAL strongly correlated with mortality ( r = 0.48, P = 0.004) and all measures of morbidity mentioned above.
Related collections
Most cited references28
- Record: found
- Abstract: found
- Article: not found
Minimal changes of serum creatinine predict prognosis in patients after cardiothoracic surgery: a prospective cohort study.
- Record: found
- Abstract: found
- Article: not found
A clinical score to predict acute renal failure after cardiac surgery.
- Record: found
- Abstract: found
- Article: not found