- Record: found
- Abstract: found
- Article: found
Cardiac Output Measurements in Septic Patients: Comparing the Accuracy of USCOM to PiCCO
Read this article at
Abstract
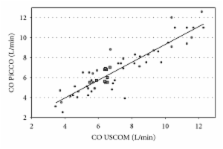
USCOM is an ultrasound-based method which has been accepted for noninvasive hemodynamic monitoring in various clinical conditions (USCOM, Ultrasonic cardiac output monitoring). The present study aimed at comparing the accuracy of the USCOM device with that of the thermodilution technique in patients with septicemia. We conducted a prospective observational study in a medical but noncardiological ICU of a university hospital. Septic adult patients (median age 55 years, median SAPS-II-Score 43 points) on mechanical ventilation and catecholamine support were monitored with USCOM and PiCCO ( n = 70). Seventy paired left-sided CO measurements (transaortic access = CO US-A) were obtained. The mean CO US-A were 6.55 l/min (±2.19) versus CO PiCCO 6.5 l/min (±2.18). The correlation coefficient was r = 0.89. Comparison by Bland-Altman analysis revealed a bias of −0.36 l/min (±0.99 l/min) leading to a mean percentage error of 29%. USCOM is a feasible and rapid method to evaluate CO in septic patients. USCOM does reliably represent CO values as compared to the reference technique based on thermodilution (PiCCO). It seems to be appropriate in situations where CO measurements are most pertinent to patient management.
Related collections
Most cited references31
- Record: found
- Abstract: found
- Article: not found
Estimation of left ventricular systolic function by single transpulmonary thermodilution.
- Record: found
- Abstract: found
- Article: not found
Clinical evaluation of USCOM ultrasonic cardiac output monitor in cardiac surgical patients in intensive care unit.
- Record: found
- Abstract: found
- Article: not found