- Record: found
- Abstract: found
- Article: found
Low-dose aspirin and racial disparities in spontaneous preterm delivery in low-risk individuals
Read this article at
Abstract
BACKGROUND
Preterm birth is a leading cause of perinatal morbidity and mortality. There are significant racial disparities in the rates of preterm delivery in the United States, with Black individuals at disproportionately higher risk than their White counterparts. Although low-dose aspirin is currently under investigation for reducing the rates of preterm delivery, limited data are available on how the use of low-dose aspirin might affect racial and ethnic disparities in the rates of preterm delivery.
OBJECTIVE
Our group and others have shown that low-dose aspirin decreases spontaneous preterm delivery in low-risk parturients. This study aimed to examine whether the relationship between low-dose aspirin and the risk of spontaneous preterm delivery is modified by race and ethnicity.
STUDY DESIGN
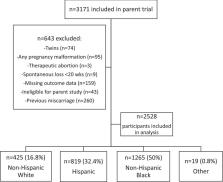
This was a secondary analysis of a randomized clinical trial examining low-dose aspirin for preeclampsia prevention in low-risk nulliparous individuals. The parent trial defined low risk as the absence of preexisting hypertension or other medical comorbidities. Participants received 60-mg aspirin or placebo between 13 and 25 weeks of gestation. Here, multiple pregnancies, fetal anomalies, terminations or abortions at <20 weeks of gestation, and participants with previous miscarriages were excluded. Our exposure, race and ethnicity, was self-reported in the parent trial and categorized as non-Hispanic White, Hispanic, non-Hispanic Black, and other. The primary outcome was spontaneous preterm delivery at <34 weeks of gestation; the secondary outcomes included spontaneous preterm delivery at <37 weeks of gestation and all preterm deliveries at <34 and <37 weeks of gestation. Fit logistic regression models were used to examine how the use of low-dose aspirin modified the relationship between race and ethnicity and preterm delivery, adjusting for confounders. Furthermore, sensitivity analyses were performed to compare the rates of preterm delivery by race and ethnicity.
RESULTS
Of note, 2528 of 3171 parent study participants were included in this analysis. Of the participants, 425 (16.8%) were White, 819 (32.4%) were Hispanic, 1265 (50%) were Black, and 19 (0.8%) were other. The baseline characteristics differed among racial and ethnic groups, including maternal age, body mass index, education level, marital status, tobacco and alcohol use, and pregnancy loss. The rate of spontaneous preterm delivery at <34 weeks of gestation was significantly higher in Black participants (2.8%) than in White (1.2%) and Hispanic (1.2%) participants ( P=.04). Logistical regression analysis showed that Black race was no longer an independent risk factor for spontaneous preterm delivery at <34 weeks of gestation when controlling for low-dose aspirin (adjusted odds ratio, 1.71; 95% confidence interval, 0.67–4.40). A similar pattern was found for spontaneous preterm delivery at <37 weeks of gestation and preterm delivery at <34 and <37 weeks of gestation. In our sensitivity analyses, spontaneous preterm delivery at <34 weeks of gestation differed by race and ethnicity in the placebo group ( P=.01) but did not differ in the low-dose aspirin group ( P=.90).
Related collections
Most cited references53
- Record: found
- Abstract: found
- Article: not found
Epidemiology and causes of preterm birth
- Record: found
- Abstract: found
- Article: not found
Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000.
- Record: found
- Abstract: found
- Article: found