- Record: found
- Abstract: found
- Article: found
Prevalence of zero-sanitation in India: Patterns of change across the states and Union Territories, 1993-2021

Read this article at
Abstract
Background
Ensuring universal access to safe sanitation by 2030 is a development priority for India. Doing so can help ensure improved physical and mental health outcomes. While the proportion of people in India with safe sanitation has risen dramatically over the past thirty years, much less is known about who has been most at risk for not having access to safe sanitation across India’s states and Union Territories (UT) over this time period. We introduce the concept of zero-sanitation to fill this gap.
Methods
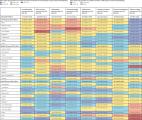
Data from five National Family Health Surveys (NFHS) conducted in 1993, 1999, 2006, 2016, and 2021 from 36 states and UT were used for this study. The study population consisted for all household individuals regardless of age in each survey round. Zero-sanitation was defined as those who have no access to a household toilet, and thus defecate in the open. We analyzed the percent prevalence of zero-sanitation in every state / UT at each time period in both urban and rural communities, as well as the population headcount burden in 2021. We calculated the absolute change on an annual basis to assess the change in percentage points of zero-sanitation across time periods at the all-India and state / UT levels.
Results
The all-India prevalence of zero-sanitation declined from 70.3% (95% confidence interval (CI) = 70.2%-70.5%) in 1993 to 17.8% (95% CI = 17.7%-17.9%) in 2021. The median percent prevalence of zero-sanitation across states and UTs was 65.9% in 1993. By 2021, the median percent prevalence of zero-sanitation across states and UTs was 5.7%. This reduction corresponded with a reduction in the between state / UT inequality in zero-sanitation. Nevertheless, as of 2021, the prevalence of zero-sanitation was still above 20% in Bihar, Jharkhand, Madhya Pradesh, Odisha, Rajasthan, and Uttar Pradesh. Additionally, as of 2021, almost 92% of individuals who were defecating in the open were experiencing zero-sanitation. Zero-sanitation remains most common in states such as Bihar, Punjab, Uttar Pradesh, and Assam. Nevertheless, at this current rate of improvement, every state and UT except for Sikkim and Chandigarh are on track to end open defecation by 2030.
Conclusions
The concept of zero-sanitation is a useful tool in helping policy makers assess the extent to which sanitation coverage remains incomplete. When viewed through this lens, we see that open defecation remains most common among those who do not have a toilet. Addressing the myriad social determinants of sanitation access can help fill these gaps and ensure equitable sanitation coverage throughout India.
Related collections
Most cited references41

- Record: found
- Abstract: found
- Article: found
Sanitation and Health

- Record: found
- Abstract: found
- Article: found
Use of quantitative molecular diagnostic methods to investigate the effect of enteropathogen infections on linear growth in children in low-resource settings: longitudinal analysis of results from the MAL-ED cohort study
- Record: found
- Abstract: found
- Article: found