- Record: found
- Abstract: found
- Article: found
Primary clear cell carcinoma of the vulva: A case report
Read this article at
Highlights
-
•
Unlike clear cell carcinoma of the endometrium or ovary, clear cell carcinoma of the vulva is an extremely rare and poorly understood disease.
-
•
The majority of reported cases arise from endometriosis or from the Bartholin’s gland.
-
•
We describe a case of clear cell carcinoma of the vulva likely arising from endometriosis.
Abstract
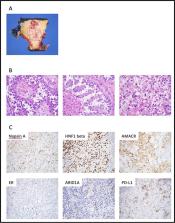
Clear cell carcinoma (CCC) of the vulva is extremely rare. We report a case of a 54-year-old woman who presented with a 5 cm mass of the mons pubis. She underwent needle biopsy demonstrating CCC. She then underwent radical vulvectomy with bilateral inguinofemoral lymph node dissection. Surgical pathology revealed CCC of the vulva with lymphovascular space invasion (LVSI) and metastatic carcinoma in 1/7 inguinal lymph nodes. The patient has a history of endometriosis, raising suspicion that her CCC could have arisen from endometriosis in the mons. She completed adjuvant treatment with cisplatin and concurrent external beam radiation therapy with radiographic evidence of complete response. However, short-interval imaging demonstrated multi-focal recurrence, which was confirmed with supraclavicular lymph node biopsy. She then completed 8 cycles carboplatin, paclitaxel, and biosimilar bevacizumab-bvzr with favorable response on imaging. She was continued on bevacizumab maintenance. She was later started on pembroluzimab for disease progression based on new mediastinal adenopathy and worsening retroperitoneal lymphadenopathy. She received eight cycles of pembrolizumab with ongoing disease progression before enrolling in hospice and discontinuing cancer-directed treatment. As described in the related literature which we summarize here, the majority of reported cases of vulvar CCC arise from endometriosis implants at the site of prior episiotomy or from the Bartholin’s gland. This patient had clinical history of endometriosis; prior tissue sampling was not performed to support the diagnosis. Given the absence of data regarding this rare type of primary vulvar cancer, treatment of this patient’s disease was based on existing data specific to squamous cell carcinoma of the vulva and extrapolated from treatment guidelines for CCC of the ovary and endometrium. Continued research is needed on this rare form of vulvar carcinoma to determine the risk factors, prognostic factors, and treatment recommendations specific to this disease.
Related collections
Most cited references19
- Record: found
- Abstract: found
- Article: not found
ARID1A mutations in endometriosis-associated ovarian carcinomas.
- Record: found
- Abstract: not found
- Article: not found
ENDOMETRIAL CARCINOMA OF THE OVARY, ARISING IN ENDOMETRIAL TISSUE IN THAT ORGAN
- Record: found
- Abstract: found
- Article: found