- Record: found
- Abstract: found
- Article: found
Treatment of behavioral and psychological symptoms of dementias with psychopharmaceuticals: a review
Abstract
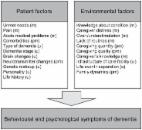
Behavioral and psychological symptoms represent common complications in patients with different types of dementia. Predominantly, they comprise psychosis, agitation and mood disorders, disinhibited behavior, impairment of the sleep and wakefulness rhythm, wandering, perseveration, pathological collecting, or shouting. Their appearance is related to more rapid progression of the disease, earlier institutionalization, use of physical restraints, and higher risk of mortality. Consequently, appearance of behavioral and psychological symptoms of dementia leads to higher costs of care provided and greater distress for caregivers. Clinical guidelines recommend nonpharmacological approaches as the first choice in the treatment of behavioral and psychological symptoms. Pharmacological therapy should be initiated only if the symptoms were not the result of somatic causes, did not respond to nonpharmacological interventions, or were not caused by the prior medication. Acetylcholinesterase inhibitors, memantine, antipsychotic drugs, antidepressants, mood stabilizers, and benzodiazepines are used. This review summarizes the current findings about the efficacy and safety of the treatment of the neuropsychiatric symptoms in dementias with psychopharmaceuticals. Recommendations for treatment with antipsychotics for this indication are described in detail as this drug group is prescribed most often and, at the same time, is related to the highest risk of adverse effects and increased mortality.
Most cited references53
- Record: found
- Abstract: found
- Article: not found
The dementia antipsychotic withdrawal trial (DART-AD): long-term follow-up of a randomised placebo-controlled trial.
- Record: found
- Abstract: not found
- Article: not found
The American Psychiatric Association Practice Guideline on the Use of Antipsychotics to Treat Agitation or Psychosis in Patients With Dementia.
- Record: found
- Abstract: found
- Article: found