- Record: found
- Abstract: found
- Article: found
Age and sex differences in the effects of short- and long-term exposure to air pollution on endothelial dysfunction
Read this article at
Abstract
Background
The effects of air pollution on endothelial function remain unclear across populations. We aimed to use brachial artery flow-mediated dilatation (FMD) to identify demographic differences in the effects of air pollution exposure on endothelial dysfunction.
Methods
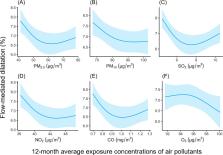
We measured FMD in 850 participants from October 2016 to January 2020. Location-specific concentrations of fine particulate matter < 2.5 μm aerodynamic diameter (PM 2.5), inhalable particulate matter < 10 μm aerodynamic diameter (PM 10), sulfur dioxide (SO 2), nitrogen dioxide (NO 2), carbon monoxide (CO), and ozone (O 3) measured by fixed ambient air monitoring stations were collected for short- and long-term exposure assessment. Multiple linear regression models and restricted cubic splines were used to assess the associations before and after stratification by age and sex.
Results
This study eventually included 828 participants [551 (66.5%) younger than 65 years and 553 (66.8%) men]. Each 10 µg/m 3 increase in 7-day exposure to PM 2.5 and PM 10 was significantly linearly associated with a 0.07% ( β = -0.07, 95% CI: -0.13 to -0.004) and 0.05% ( β = -0.05, 95% CI: -0.10 to -0.004) decrease in FMD in the fully adjusted model. After full adjustment, long-term exposure to all air pollutants was significantly associated with impaired FMD. Each 10 µg/m 3 increase in long-term exposure to PM 2.5 and PM 10 was significantly associated with a -0.18% (95% CI: -0.34 to -0.03) and − 0.23% (95% CI: -0.40 to -0.06) change in FMD, respectively. After stratification, the associations of lower FMD with long-term exposure to PM 2.5, PM 10, SO 2, NO 2, and CO significantly persisted in men and participants younger than 65 years instead of women or older participants. For short-term exposure, we observed differences consistent with long-term exposure and a stronger effect of 7-day exposure to SO 2 in men due to a significant interaction effect.
Related collections
Most cited references33

- Record: found
- Abstract: found
- Article: found
Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019

- Record: found
- Abstract: found
- Article: found
Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017

- Record: found
- Abstract: found
- Article: found