- Record: found
- Abstract: found
- Article: not found
Higher dose corticosteroids in patients admitted to hospital with COVID-19 who are hypoxic but not requiring ventilatory support (RECOVERY): a randomised, controlled, open-label, platform trial
Read this article at
- open (via crossref license)
- oa repository (via OAI-PMH doi match)
- oa repository (via OAI-PMH doi match)
- oa repository (via OAI-PMH doi match)
- oa repository (via OAI-PMH doi match)
- oa repository (via OAI-PMH doi match)
- oa repository (via OAI-PMH doi match)
- oa repository (via OAI-PMH doi match)
- oa repository (via OAI-PMH title and first author match)
- oa repository (via OAI-PMH title and first author match)
- oa repository (via pmcid lookup)
- oa repository (via OAI-PMH doi match)
- oa repository (via OAI-PMH doi match)
- oa repository (via OAI-PMH doi match)
- oa repository (via OAI-PMH doi match)
- oa repository (via OAI-PMH doi match)
Powered by 
Abstract
Background
Low-dose corticosteroids have been shown to reduce mortality for patients with COVID-19 requiring oxygen or ventilatory support (non-invasive mechanical ventilation, invasive mechanical ventilation, or extracorporeal membrane oxygenation). We evaluated the use of a higher dose of corticosteroids in this patient group.
Methods
This randomised, controlled, open-label platform trial (Randomised Evaluation of COVID-19 Therapy [RECOVERY]) is assessing multiple possible treatments in patients hospitalised for COVID-19. Eligible and consenting adult patients with clinical evidence of hypoxia (ie, receiving oxygen or with oxygen saturation <92% on room air) were randomly allocated (1:1) to either usual care with higher dose corticosteroids (dexamethasone 20 mg once daily for 5 days followed by 10 mg dexamethasone once daily for 5 days or until discharge if sooner) or usual standard of care alone (which included dexamethasone 6 mg once daily for 10 days or until discharge if sooner). The primary outcome was 28-day mortality among all randomised participants. On May 11, 2022, the independent data monitoring committee recommended stopping recruitment of patients receiving no oxygen or simple oxygen only due to safety concerns. We report the results for these participants only. Recruitment of patients receiving ventilatory support is ongoing. The RECOVERY trial is registered with ISRCTN (50189673) and ClinicalTrials.gov (NCT04381936).
Findings
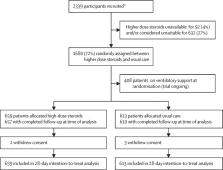
Between May 25, 2021, and May 13, 2022, 1272 patients with COVID-19 and hypoxia receiving no oxygen (eight [1%]) or simple oxygen only (1264 [99%]) were randomly allocated to receive usual care plus higher dose corticosteroids (659 patients) versus usual care alone (613 patients, of whom 87% received low-dose corticosteroids during the follow-up period). Of those randomly assigned, 745 (59%) were in Asia, 512 (40%) in the UK, and 15 (1%) in Africa. 248 (19%) had diabetes and 769 (60%) were male. Overall, 123 (19%) of 659 patients allocated to higher dose corticosteroids versus 75 (12%) of 613 patients allocated to usual care died within 28 days (rate ratio 1·59 [95% CI 1·20–2·10]; p=0·0012). There was also an excess of pneumonia reported to be due to non-COVID infection (64 cases [10%] vs 37 cases [6%]; absolute difference 3·7% [95% CI 0·7–6·6]) and an increase in hyperglycaemia requiring increased insulin dose (142 [22%] vs 87 [14%]; absolute difference 7·4% [95% CI 3·2–11·5]).
Interpretation
In patients hospitalised for COVID-19 with clinical hypoxia who required either no oxygen or simple oxygen only, higher dose corticosteroids significantly increased the risk of death compared with usual care, which included low-dose corticosteroids. The RECOVERY trial continues to assess the effects of higher dose corticosteroids in patients hospitalised with COVID-19 who require non-invasive ventilation, invasive mechanical ventilation, or extracorporeal membrane oxygenation.
Related collections
Most cited references17
- Record: found
- Abstract: found
- Article: not found
Dexamethasone in Hospitalized Patients with Covid-19 — Preliminary Report
- Record: found
- Abstract: found
- Article: found
Association Between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19: A Meta-analysis
- Record: found
- Abstract: found
- Article: not found