- Record: found
- Abstract: found
- Article: found
CX3CL1/CX3CR1 Axis, as the Therapeutic Potential in Renal Diseases: Friend or Foe?
Read this article at
Abstract
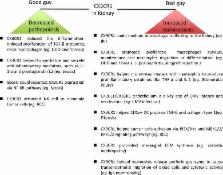
The fractalkine receptor chemokine (C-X3-C motif) receptor 1 (CX3CR1) and its highly se-lective ligand CX3CL1 mediate chemotaxis and adhesion of immune cells, which are involved in the pathogenesis and progression of numerous inflammatory disorders and malignancies. The CX3CL1/CX3CR1 axis has recently drawn attention as a potential therapeutic target because it is in-volved in the ontogeny, homeostatic migration, or colonization of renal phagocytes. We performed a Medline/PubMed search to detect recently published studies that explored the relationship between the CX3CL1/CX3CR1 axis and renal diseases and disorders, including diabetic nephropathy, renal allograft rejection, infectious renal diseases, IgA nephropathy, fibrotic kidney disease, lupus nephritis and glo-merulonephritis, acute kidney injury and renal carcinoma. Most studies demonstrated its role in promot-ing renal pathopoiesis; however, several recent studies showed that the CX3CL1/CX3CR1 axis could also reduce renal pathopoiesis. Thus, the CX3CL1/CX3CR1 axis is now considered to be a double-edged sword that could provide novel perspectives into the pathogenesis and treatment of renal diseases and disorders.
Related collections
Most cited references79
- Record: found
- Abstract: found
- Article: not found