- Record: found
- Abstract: found
- Article: found
Combined Perfusion and Permeability Imaging Reveals Different Pathophysiologic Tissue Responses After Successful Thrombectomy
Read this article at
Abstract
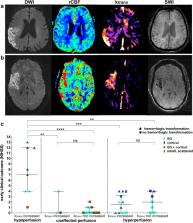
Despite successful recanalization of large-vessel occlusions in acute ischemic stroke, individual patients profit to a varying degree. Dynamic susceptibility-weighted perfusion and dynamic T1-weighted contrast-enhanced blood-brain barrier permeability imaging may help to determine secondary stroke injury and predict clinical outcome. We prospectively performed perfusion and permeability imaging in 38 patients within 24 h after successful mechanical thrombectomy of an occlusion of the middle cerebral artery M1 segment. Perfusion alterations were evaluated on cerebral blood flow maps, blood-brain barrier disruption (BBBD) visually and quantitatively on k trans maps and hemorrhagic transformation on susceptibility-weighted images. Visual BBBD within the DWI lesion corresponded to a median k trans elevation (IQR) of 0.77 (0.41–1.4) min −1 and was found in all 7 cases of hypoperfusion (100%), in 10 of 16 cases of hyperperfusion (63%), and in only three of 13 cases with unaffected perfusion (23%). BBBD was significantly associated with hemorrhagic transformation ( p < 0.001). While BBBD alone was not a predictor of clinical outcome at 3 months (positive predictive value (PPV) = 0.8 [0.56–0.94]), hypoperfusion occurred more often in patients with unfavorable clinical outcome (PPV = 0.43 [0.10–0.82]) compared to hyperperfusion (PPV = 0.93 [0.68–1.0]) or unaffected perfusion (PPV = 1.0 [0.75–1.0]). We show that combined perfusion and permeability imaging reveals distinct infarct signatures after recanalization, indicating the severity of prior ischemic damage. It assists in predicting clinical outcome and may identify patients at risk of stroke progression.
Related collections
Most cited references45
- Record: found
- Abstract: found
- Article: not found
User-guided 3D active contour segmentation of anatomical structures: significantly improved efficiency and reliability.
- Record: found
- Abstract: not found
- Article: not found
Improved Optimization for the Robust and Accurate Linear Registration and Motion Correction of Brain Images
- Record: found
- Abstract: found
- Article: not found