- Record: found
- Abstract: found
- Article: found
Tumor budding, a novel prognostic indicator for predicting stage progression in T1 bladder cancers

Read this article at
Abstract
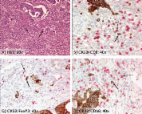
Tumor budding has been defined as an isolated single cancer cell or a cluster composed of fewer than five cancer cells scattered in the stroma. It is a strong predictor for lymph node metastasis in T1 colorectal cancer. We introduced this concept to T1 non‐muscle invasive bladder cancer and evaluated whether tumor budding could have a prognostic impact on the clinical outcome. We identified 121 consecutive patients with newly diagnosed T1 bladder cancer between 1994 and 2014 at Keio University Hospital. All slides were re‐reviewed by a dedicated uropathologist. Budding foci were counted under ×200 magnification. When the number of budding foci was 10 or more, tumor budding was defined as positive. The relationship between tumor budding and clinical outcomes was assessed using a multivariate analysis. The median follow‐up was 52 months. Tumor budding was positive in 21 patients (17.4%). Tumor budding was significantly associated with T1 substaging, tumor architecture and lymphovascular invasion. The 5‐year progression‐free survival rate in T1 bladder cancer patients with tumor budding was 53.8%, which was significantly lower than that in patients without tumor budding (88.4%, P = 0.001). A multivariate Cox regression analysis revealed that tumor budding was independently associated with stage progression ( P = 0.002, hazard ratio = 4.90). In a subgroup of patients treated with bacillus Calmette‐Guérin instillation ( n = 88), tumor budding was also independently associated with stage progression ( P = 0.003, hazard ratio = 5.65). Tumor budding may be a novel indicator for predicting stage progression in T1 bladder cancer, and would likely be easily introduced in clinical practice.
Related collections
Most cited references23
- Record: found
- Abstract: found
- Article: not found
Japanese Society for Cancer of the Colon and Rectum (JSCCR) Guidelines 2014 for treatment of colorectal cancer
- Record: found
- Abstract: found
- Article: not found
Risk factors for an adverse outcome in early invasive colorectal carcinoma.
- Record: found
- Abstract: found
- Article: found