- Record: found
- Abstract: found
- Article: found
Predictive nomogram models for unfavorable prognosis after aneurysmal subarachnoid hemorrhage: Analysis from a prospective, observational cohort in China

Read this article at
Abstract
Aim
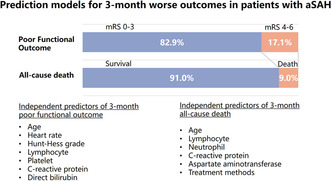
The aim of the study was to identify predictors for 3‐month poor functional outcome or death after aSAH and develop precise and easy‐to‐use nomogram models.
Methods
The study was performed at the department of neurology emergency in Beijing Tiantan Hospital. A total of 310 aSAH patients were enrolled between October 2020 and September 2021 as a derivation cohort, while a total of 208 patients were admitted from October 2021 to March 2022 as an external validation cohort. Clinical outcomes included poor functional outcome defined as modified Rankin Scale score (mRS) of 4–6 or all‐cause death at 3 months. Least absolute shrinkage and selection operator (LASSO) analysis, as well as multivariable regression analysis, were applied to select independent variables associated with poor functional outcome or death and then to construct two nomogram models. Model performance were evaluated through discrimination, calibration, and clinical usefulness in both derivation cohort and external validation cohort.
Results
The nomogram model to predict poor functional outcome included seven predictors: age, heart rate, Hunt‐Hess grade on admission, lymphocyte, C‐reactive protein (CRP), platelet, and direct bilirubin levels. It demonstrated high discrimination ability (AUC, 0.845; 95% CI: 0.787–0.903), satisfactory calibration curve, and good clinical usefulness. Similarly, the nomogram model combining age, neutrophil, lymphocyte, CRP, aspartate aminotransferase (AST) levels, and treatment methods to predict all‐cause death also revealed excellent discrimination ability (AUC, 0.944; 95% CI: 0.910–0.979), satisfactory calibration curve, and clinical effectiveness. Internal validation showed the bias‐corrected C‐index for poor functional outcome and death was 0.827 and 0.927, respectively. When applied to the external validation dataset, both two nomogram models exhibited high discrimination capacity [poor functional outcome: AUC = 0.795 (0.716–0.873); death: AUC = 0.811 (0.707–0.915)], good calibration ability, and clinical usefulness.
Conclusions
Nomogram models constructed for predicting 3‐month poor functional outcome or death after aSAH are precise and easily applicable, which can help physicians to identify patients at risk, guide decision‐making, and provide new directions for future studies to explore the novel treatment targets.
Abstract
We constructed precise and easily applicable nomogram models to predict 3‐month poor functional outcome or death after aSAH. These prediction models can help physicians to identify patients at risk, guide decision‐making, and provide new directions for future studies to explore the novel treatment targets.
Related collections
Most cited references47
- Record: found
- Abstract: found
- Article: not found
Nomograms in oncology: more than meets the eye.
- Record: found
- Abstract: found
- Article: not found
Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/american Stroke Association.
- Record: found
- Abstract: found
- Article: not found