- Record: found
- Abstract: found
- Article: found
Dietary intake and biomarkers of alpha linolenic acid and risk of all cause, cardiovascular, and cancer mortality: systematic review and dose-response meta-analysis of cohort studies
Read this article at
Abstract
Objective
To examine the associations between dietary intake and tissue biomarkers of alpha linolenic acid (ALA) and risk of mortality from all causes, cardiovascular disease (CVD), and cancer.
Study selection
Prospective cohort studies that reported the risk estimates for death from all causes, CVD, and cancer.
Data synthesis
Summary relative risks and 95% confidence intervals were calculated for the highest versus lowest categories of ALA intake using random effects and fixed effects models. Linear and non-linear dose-response analyses were conducted to assess the dose-response associations between ALA intake and mortality.
Results
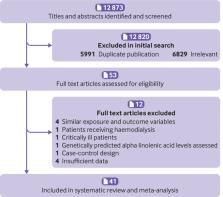
41 articles from prospective cohort studies were included in this systematic review and meta-analysis, totalling 1 197 564 participants. During follow-up ranging from two to 32 years, 198 113 deaths from all causes, 62 773 from CVD, and 65 954 from cancer were recorded. High intake of ALA compared with low intake was significantly associated with a lower risk of deaths from all causes (pooled relative risk 0.90, 95% confidence interval 0.83 to 0.97, I 2=77.8%, 15 studies), CVD (0.92, 0.86 to 0.99, I 2=48.2%, n=16), and coronary heart disease (CHD) (0.89, 0.81 to 0.97, I 2=5.6%, n=9), and a slightly higher risk of cancer mortality (1.06, 1.02 to 1.11, I 2=3.8%, n=10). In the dose-response analysis, a 1 g/day increase in ALA intake (equivalent to one tablespoon of canola oil or 0.5 ounces of walnut) was associated with a 5% lower risk of all cause (0.95, 0.91 to 0.99, I 2=76.2%, n=12) and CVD mortality (0.95, 0.91 to 0.98, I 2=30.7%, n=14). The pooled relative risks for the highest compared with lowest tissue levels of ALA indicated a significant inverse association with all cause mortality (0.95, 0.90 to 0.99, I 2=8.2%, n=26). Also, based on the dose-response analysis, each 1 standard deviation increment in blood concentrations of ALA was associated with a lower risk of CHD mortality (0.92, 0.86 to 0.98, I 2=37.1%, n=14).
Related collections
Most cited references102
- Record: found
- Abstract: found
- Article: not found
Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012.
- Record: found
- Abstract: not found
- Article: not found