Acceptance, Hesitancy, and Refusal Among Parents of Young Girls in Relation to Human Papillomavirus Vaccination: A Study From the Mohammed VI University Hospital Center in Oujda, Morocco
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
Introduction: Morocco has joined the global efforts to eliminate cervical cancer by
introducing human papillomavirus (HPV) vaccination into its national immunization
program. However, vaccination rates remain insufficient relative to the importance
of the vaccine. Therefore, the objective of the study was to understand better the
factors associated with acceptance, hesitance, or refusal of the HPV vaccine.
Materials and methods: A descriptive and analytical study was conducted among 450
parents of girls of HPV vaccination age at the Mohammed VI University Hospital Center
in Oujda, Morocco, over a period of three months.
Results: A total of 450 parents were included in the study, most of them being mothers.
Most parents were unaware of HPV infection (66%) or the HPV vaccine (62%). The rate
of HPV vaccination among the study population was only 33%. Factors associated with
nonvaccination included a lack of information about the HPV vaccine (57%), concern
about side effects (33%), and unvaccinated family and friends (10%). Parents’ intention
to vaccinate their daughters was significantly lower in fathers (95% confidence interval,
or 95% CI = 0.34-0.66), those with a low educational level (odds ratio, or OR = 0.53;
95% CI = 0.40-0.80), and those with an unfavorable socioeconomic level (OR = 0.41;
95% CI = 0.30-0.56), whereas it was significantly higher in cases of a vaccinated
entourage, including friends and family (OR = 1.52; 95% CI = 1.22-2.12), and when
vaccination was recommended by a doctor (OR = 1.92; 95% CI = 1.56-2.39).
Conclusion: The results of our study highlighted parents’ lack of information about
HPV infection and the HPV vaccine. They also revealed a clear lack of HPV vaccination
coverage and identified the reasons for reluctance to vaccinate against HPV. Much
remains to be done to increase the rate of HPV vaccination in Morocco.
Three vaccines are recommended by the Advisory Committee on Immunization Practices (ACIP) for routine vaccination of adolescents aged 11–12 years to protect against 1) pertussis; 2) meningococcal disease caused by types A, C, W, and Y; and 3) human papillomavirus (HPV)-associated cancers ( 1 ). At age 16 years, a booster dose of quadrivalent meningococcal conjugate vaccine (MenACWY) is recommended. Persons aged 16–23 years can receive serogroup B meningococcal vaccine (MenB), if determined to be appropriate through shared clinical decision-making. CDC analyzed data from the 2019 National Immunization Survey-Teen (NIS-Teen) to estimate vaccination coverage among adolescents aged 13–17 years in the United States.* Coverage with ≥1 dose of HPV vaccine increased from 68.1% in 2018 to 71.5% in 2019, and the percentage of adolescents who were up to date † with the HPV vaccination series (HPV UTD) increased from 51.1% in 2018 to 54.2% in 2019. Both HPV vaccination coverage measures improved among females and males. An increase in adolescent coverage with ≥1 dose of MenACWY (from 86.6% in 2018 to 88.9% in 2019) also was observed. Among adolescents aged 17 years, 53.7% received the booster dose of MenACWY in 2019, not statistically different from 50.8% in 2018; 21.8% received ≥1 dose of MenB, a 4.6 percentage point increase from 17.2% in 2018. Among adolescents living at or above the poverty level, § those living outside a metropolitan statistical area (MSA) ¶ had lower coverage with ≥1 dose of MenACWY and with ≥1 HPV vaccine dose, and a lower percentage were HPV UTD, compared with those living in MSA principal cities. In early 2020, the coronavirus disease 2019 (COVID-19) pandemic changed the way health care providers operate and provide routine and essential services. An examination of Vaccines for Children (VFC) provider ordering data showed that vaccine orders for HPV vaccine; tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis vaccine (Tdap); and MenACWY decreased in mid-March when COVID-19 was declared a national emergency (Supplementary Figure 1, https://stacks.cdc.gov/view/cdc/91795). Ensuring that routine immunization services for adolescents are maintained or reinitiated is essential to continuing progress in protecting persons and communities from vaccine-preventable diseases and outbreaks. NIS-Teen is a random-digit-dial telephone survey** conducted annually to monitor vaccination coverage among adolescents aged 13–17 years in the 50 states, the District of Columbia, selected local areas, and selected U.S. territories. †† Sociodemographic information is collected during the telephone interview with a parent or guardian, and a request is made for consent to contact the adolescent’s vaccination provider(s). If consent is obtained, a questionnaire is mailed to the vaccination provider(s) to request the adolescent’s vaccination history. Vaccination coverage estimates are determined from these provider-reported immunization records. This report provides vaccination coverage estimates on 18,788 adolescents aged 13–17 years. §§ The overall Council of American Survey Research Organizations (CASRO) ¶¶ response rate was 19.7%, and 44.0% of adolescents for whom household interviews were completed had adequate provider data. Data were weighted and analyzed to account for the complex sampling design.*** T-tests were used to assess vaccination coverage differences between sociodemographic subgroups. P-values 20 might not be reliable. § Includes percentages receiving Tdap at age ≥10 years. ¶ Statistically significant difference (p 20 might not be reliable. ¶ Includes percentages receiving Tdap at age ≥10 years. ** Includes percentages receiving MenACWY and meningococcal-unknown type vaccine. †† Statistically significant difference (p<0.05) in estimated vaccination coverage by MSA; referent group was adolescents living in MSA principal city areas. §§ ≥2 doses of MenACWY or meningococcal-unknown type vaccine. Calculated only among adolescents aged 17 years at interview. Does not include adolescents who received 1 dose of MenACWY at age ≥16 years. ¶¶ HPV vaccine, nine-valent (9vHPV), quadrivalent (4vHPV), or bivalent (2vHPV). *** HPV UTD includes those who’ve received ≥3 doses and those with 2 doses when the first HPV vaccine dose was initiated before age 15 years and there was at least 5 months minus 4 days between the first and second dose. This update to the HPV recommendation occurred in December of 2016. ††† In July 2020, ACIP revised recommendations for Hepatitis A vaccination to include catch-up vaccination for children and adolescents aged 2–18 years who have not previously received Hepatitis A vaccine at any age (http://dx.doi.org/10.15585/mmwr.rr6905a1). §§§ By parent/guardian report or provider records. Trends in HPV Vaccination by Birth Cohort HPV vaccination initiation by age 13 years increased an average of 5.3 percentage points for each consecutive birth year, from 19.9% among adolescents born in 1998 to 62.6% among those born in 2006 (Supplementary Figure 2, https://stacks.cdc.gov/view/cdc/91796). Being HPV UTD by age 13 years increased an average of 3.4 percentage points for each consecutive birth year, from 8.0% among adolescents born in 1998 to 35.5% among those born in 2006. Discussion In 2019, coverage with HPV vaccine and with MenACWY improved compared with coverage in 2018. Improvements in ≥1 dose HPV and HPV UTD vaccination coverage were observed among females and males. In addition, more teens began HPV vaccination on time (by age 13 years) in 2019, suggesting that more parents are making the decision to protect their teens against HPV-associated cancers. Efforts from federal, state, and other stakeholders to prioritize HPV vaccination among adolescents, and reducing the number of recommended HPV vaccine doses from a 3-dose to a 2-dose series ( 2 ), likely contributed to these improvements. Coverage with ≥1 dose of MenACWY increased to 88.9%; coverage with ≥2 doses remained low at 53.7%, indicating that continued efforts are needed to improve receipt of the booster dose. Despite progress in adolescent HPV vaccination and MenACWY coverage, disparities remain; all adolescents are not equally protected against vaccine-preventable diseases. As in previous years, compared with adolescents living in MSA principal cities, HPV UTD status and coverage with ≥1 dose each of HPV vaccine and MenACWY continue to be lower among adolescents in non-MSA areas ( 3 ). However, these geographic disparities were present only for adolescents at or above the poverty level in 2019. This finding is consistent with another study that found socioeconomic status to be a moderating factor in the association between HPV vaccination and MSA ( 4 ). The lack of an MSA disparity among adolescents below the poverty level might reflect the access that low-income adolescents have to the VFC program****; previous studies have reported higher HPV vaccination coverage rates among adolescents living below the poverty level ( 5 , 6 ). Reasons for the MSA disparity among higher socioeconomic status adolescents are less clear but might be an indicator of lower vaccine confidence. More work is needed to understand the relationship between socioeconomic status and geographic disparities and the barriers that might be contributing to such differences. The findings in this report are subject to at least two limitations. First, the CASRO response rate to NIS-Teen was 19.7%, and only 44.0% of households with completed interviews had adequate provider data. A portion of the questionnaires sent to vaccination provider(s) to request the adolescent’s vaccination history were mailed in early 2020. A lower response rate was observed for those requests, likely because of the effect of the COVID-19 pandemic on health care provider operations. †††† Second, even with adjustments for household and provider nonresponse, landline-only households, and phoneless households, a bias in the estimates might remain. §§§§ The COVID-19 pandemic has the potential to offset historically high vaccination coverage with Tdap and MenACWY and to reverse gains made in HPV vaccination coverage. Orders for adolescent vaccines have decreased among VFC providers during the pandemic. A recent analysis using VFC provider ordering data showed a decline in vaccine orders for several VFC-funded noninfluenza childhood vaccines since mid-March when COVID-19 was declared a national emergency ( 7 ). CDC, along with other national health organizations, continues to stress the importance of well-child visits and vaccinations as essential services ( 8 ). The majority of practices appear to be open and resuming vaccination activities for their pediatric patients ( 9 , 10 ). Providers can take several steps to ensure that adolescents are up to date with recommended vaccines. These include 1) promoting well-child and vaccination visits; 2) following guidance on safely providing vaccinations during the COVID-19 pandemic ¶¶¶¶ ; 3) leveraging reminder and recall systems to remind parents of their teen’s upcoming appointment, and recalling those who missed appointments and vaccinations; and 4) educating eligible patients and parents, especially those who might have lost employer-funded insurance benefits, about the availability of publicly funded vaccines through the VFC program. In addition, state, local, and territorial immunization programs can consider using available immunization information system data***** to identify local areas and sociodemographic groups at risk for undervaccination related to the pandemic, and to help prioritize resources aimed at improving adolescent vaccination coverage. Summary What is already known about this topic? Three vaccines are routinely recommended for adolescents to prevent diseases that include pertussis, meningococcal disease, and cancers caused by human papillomavirus (HPV). What is added by this report? Adolescent vaccination coverage in the United States continues to improve for HPV and for meningococcal vaccines, with some disparities. Among adolescents living at or above the poverty level, those living outside a metropolitan statistical area (MSA) had lower coverage with HPV and meningococcal vaccines than did those living in MSA principal cities. What are the implications for public health care? Ensuring routine immunization services for adolescents, even during the COVID-19 pandemic, is essential to continuing progress in protecting individuals and communities from vaccine-preventable diseases and outbreaks.
Assessing and understanding the health needs and capacities of college students is paramount to creating healthy campus communities. The American College Health Association-National College Health Assessment (ACHA-NCHA) is a survey that ACHA developed in 1998 to assist institutions of higher education in achieving this goal. The ACHA-NCHA contains approximately 300 questions assessing student health status and health problems, risk and protective behaviors, and impediments to academic performance. The spring 2008 reference group includes ACHA-NCHA data from 80,121 students at 106 institutions of higher education. Officials at participating institutions administered the ACHA-NCHA to all students, randomly selected students, or students in randomly selected classrooms. ACHA collected data between January and May 2008. Results from the spring 2008 reference group (N=80,121) are presented. These data expand the understanding of the health needs and capacities of college students.
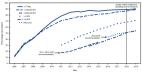
Background The proportion of incident cases of HPV-attributable cancers is highest in the low- and middle-income countries (LMICs) but many are yet to initiate HPV vaccination programs. This meta-analysis was performed to assess the uptake of HPV vaccination in LMICs at the beginning of the global strategy to eliminate cervical cancer and describes the gaps and challenges. Methods A systematic search was conducted in PubMed, EMBASE, Scopus, Web of Science, and CENTRAL databases for observational studies that reported the uptake of HPV vaccination until October 2020. The meta-analysis was done using a random-effects model to assess the pooled estimate of HPV uptake. CRD42021218429 Findings During 2008–2020, an estimated 3.3 million females received at least one dose of HPV vaccine with 61.69% of the target population vaccinated. In countries with high uptake, the pooled estimate of uptake was higher in females than males (45.48% vs 8.45%) and showed significant decline in 2015–2020 compared to 2006–2014 (89.03% vs 41.48%). In countries with low uptake, the estimate of uptake was low in both males and females (5.31% vs 2.93%) and showed increase in uptake in 2015–2020 compared to 2006–2014 (0.76% vs 5.22%). In countries with high uptake, compared to routine programs, the estimate was higher when delivered through demonstration programs (89.94% vs 59.74%). Interpretation The major concern was a significant drop in the uptake in countries that started with high uptake, challenges in the maintenance of vaccine uptake, sustainability of funding and the lack of standard monitoring and reporting.
This is an open access article distributed under the terms of the Creative Commons
Attribution License CC-BY 4.0., which permits unrestricted use, distribution, and
reproduction in any medium, provided the original author and source are credited.
scite shows how a scientific paper has been cited by providing the context of the citation, a classification describing whether it supports, mentions, or contrasts the cited claim, and a label indicating in which section the citation was made.