- Record: found
- Abstract: found
- Article: found
Obesity Paradox and Functional Outcomes in Sepsis: A Multicenter Prospective Study
Read this article at
OBJECTIVES:
In Asian populations, the correlation between sepsis outcomes and body mass is unclear. A multicenter, prospective, observational study conducted between September 2019 and December 2020 evaluated obesity’s effects on sepsis outcomes in a national cohort.
PATIENTS:
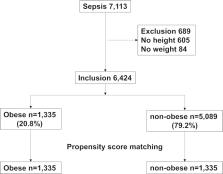
Adult patients with sepsis ( n = 6,424) were classified into obese ( n = 1,335) and nonobese groups ( n = 5,089).
MEASUREMENTS AND RESULTS:
Obese and nonobese patients were propensity score-matched in a ratio of 1:1. Inhospital mortality was the primary outcome. After propensity score matching, the nonobese group had higher hospital mortality than the obese group (25.3% vs 36.7%; p < 0.001). The obese group had a higher home discharge rate (70.3% vs 65.2%; p < 0.001) and lower median Clinical Frailty Scale (CFS) (4 vs 5; p = 0.007) at discharge than the nonobese group, whereas the proportion of frail patients at discharge (CFS ≥ 5) was significantly higher in the nonobese group (48.7% vs 54.7%; p = 0.011). Patients were divided into four groups according to the World Health Organization body mass index (BMI) classification and performed additional analyses. The adjusted odds ratio of hospital mortality and frailty at discharge for underweight, overweight, and obese patients relative to normal BMI was 1.25 ( p = 0.004), 0.58 ( p < 0.001), and 0.70 ( p = 0.047) and 1.53 ( p < 0.001), 0.80 ( p = 0.095), and 0.60 ( p = 0.022), respectively.
Related collections
Most cited references46
- Record: found
- Abstract: found
- Article: not found
Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance.
- Record: found
- Abstract: found
- Article: not found
Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: a prospective cohort study
- Record: found
- Abstract: not found
- Article: not found