- Record: found
- Abstract: found
- Article: found
Devenir néonatal immédiat de la grande et l'extrême prématurité: données rétrospectives d'une unité de néonatalogie à Yaoundé, Cameroun de 2009 à 2013 Translated title: Immediate neonatal outcome of extreme prematurity: retrospective data of a neonatal unit in Yaounde, Cameroon from 2009 to 2013
Abstract
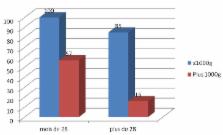
L'objectif est de notre étude de décrire la typologie de la prématurité et mesurer la survie hospitalière à court terme des grands et extrêmes prématurés dans un pays à ressources limitées (PRL). C'est une étude descriptive rétrospective. Données extraites du registre des admissions du service. Inclusions de tous les nouveau-nés admis dans le service durant la période, ayant un âge gestationnel annoncé ≤ 36 semaines et 6 jours et plus de 26SA, avec au moins deux paramètres présents: âge gestationnel et poids de naissance. Principaux paramètres mesurés: pourcentage de nouveau-nés sortants vivants selon le type de prématurité: tardive, grande ou extrême. Nous avons recensé 1015 prématurés dont 314 grands prématurés (GP) et 61 extrêmes prématurés (EP). Le taux de nouveau-nés sortant vivants était de 95% chez les prématurés tardifs, de 71% chez les grands prématurés et de moins de 23% chez les extrêmes prématurés. Avant 28 semaines, le taux de mortalité était de prés de 100% chez les grands ou extrêmes prématurés de moins de 1000g contre 64% chez les plus de 1000g. Chez les GP le taux de décès était de 13% chez les nés par césarienne vs 21% chez ceux nés par voie basse (p ≤ 0,01). Le taux de prématurité médicalement induite était faible dans l'ensemble et de 3% chez les prématurés extrêmes. En conclusion le taux de mortalité hospitalière des EP est préoccupant, le faible taux de prématurité médicalement induite urge au renforcement de la prévention et à la mise en place de collaboration obstétrico-pédiatrique.
Most cited references9
- Record: found
- Abstract: found
- Article: not found
Impact of simple interventions on neonatal mortality in a low-resource teaching hospital in India.
- Record: found
- Abstract: not found
- Article: not found
4 million neonatal deaths: When? Where? Why?
- Record: found
- Abstract: found
- Article: not found