- Record: found
- Abstract: found
- Article: found
Task sharing with non-physician health-care workers for management of blood pressure in low-income and middle-income countries: a systematic review and meta-analysis
Read this article at
Summary
Background
Task sharing for the management of hypertension could be useful for understaffed and resource-poor health systems. We assessed the effectiveness of task-sharing interventions in improving blood pressure control among adults in low-income and middle-income countries.
Methods
We searched the Cochrane Library, PubMed, Embase, and CINAHL for studies published up to December 2018. We included intervention studies involving a task-sharing strategy for management of blood pressure and other cardiovascular risk factors. We extracted data on population, interventions, blood pressure, and task sharing groups. We did a meta-analysis of randomised controlled trials.
Findings
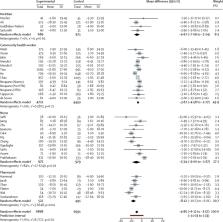
We found 3012 references, of which 54 met the inclusion criteria initially. Another nine studies were included following an updated search. There were 43 trials and 20 before-and-after studies. We included 31 studies in our meta-analysis. Systolic blood pressure was decreased through task sharing in different groups of health-care workers: the mean difference was −5·34 mm Hg (95% CI −9·00 to −1·67, I 2=84%) for task sharing with nurses, −8·12 mm Hg (–10·23 to −6·01, I 2=57%) for pharmacists, −4·67 mm Hg (–7·09 to −2·24, I 2=0%) for dietitians, −3·67 mm Hg (–4·58 to −2·77, I 2=24%) for community health workers, and −4·85 mm Hg (–6·12 to −3·57, I 2=76%) overall. We found a similar reduction in diastolic blood pressure (overall mean difference −2·92 mm Hg, −3·75 to −2·09, I 2=80%). The overall quality of evidence based on GRADE criteria was moderate for systolic blood pressure, but low for diastolic blood pressure.
Related collections
Most cited references72
- Record: found
- Abstract: found
- Article: not found
Lay health workers in primary and community health care for maternal and child health and the management of infectious diseases.
- Record: found
- Abstract: found
- Article: not found
A simple method for the analysis of clustered binary data.

- Record: found
- Abstract: found
- Article: found