- Record: found
- Abstract: found
- Article: not found
COVID–19ワクチン接種後に副腎クリーゼ,たこつぼ心筋症を発症しショックとなり多腺性自己免疫症候群2型の診断に至った1例(A patient with post COVID–19 vaccination presented with convulsions and cardiogenic shock due to adrenal crisis and Takotsubo cardiomyopathy diagnosed with autoimmune polyendocrine syndromes type II and Addison’s disease)
ABSTRACT
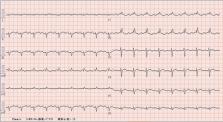
A 49–year–old woman with a history of Basedow’s disease and vitiligo during her 30s was presented with 5 days of dizziness, nausea, and fatigue after being administered the third COVID–19 vaccination and transported via emergency medical service to the emergency department with sudden loss of consciousness and convulsions. Head and whole body computed tomography were normal but laboratory examination showed severe hyponatremia, which could be the cause of severe consciousness disturbance. Similar to what is observed in Takotsubo cardiomyopathy, echocardiography revealed a mid–ventricular and apical heart–wall motion, appearing as hypokinesis; in contrast, the basal segment showed preserved features. The left ventricular dysfunction caused the progressive hypotension and cardiogenic shock. Empiric treatment with corticosteroid considering the adrenal insufficiency, mechanical circulatory support with intra–aortic balloon pumping, and proper correction of hyponatremia were effective. The patient was extubated by day 7, leading to full recovery. Additional tests confirmed the diagnosis of autoimmune polyendocrine syndromes type II (Schmidt syndrome) and Addison’s disease. This case shows that adrenal crisis is caused by the vaccine’s stress and autoimmune reaction in specific individuals. Since it is an acute life–threatening emergency, early identification and prompt management is essential.
要旨
若年時にバセドウ病,白斑病の既往のある49歳女性。COVID–19ワクチン接種後からめまい,嘔気,体動困難が出現し,5日後に意識障害,心原性ショック状態で救急搬送された。低ナトリウム血症に伴う重症意識障害,たこつぼ心筋症の診断で,挿管人工呼吸管理,電解質補正,大動脈バルーンパンピングを含む心不全治療を開始した。副腎不全を鑑別に直ちにステロイド補充を開始したところ全身状態は改善傾向となり,第7病日に抜管した。状態回復後の内分泌機能精査で,原発性副腎機能不全,多腺性自己免疫症候群2型の診断に至った。副腎クリーゼは初発だと診断がつきづらいが,重症意識障害やたこつぼ心筋症を合併し致命的となりうる重症病態であり,早期ステロイド補充が救命に不可欠である。今回,COVID–19ワクチン接種を契機に初発の副腎クリーゼを発症したが,集学的治療を行い救命しえた多腺性自己免疫症候群2型の1例を経験したため報告する。
Related collections
Most cited references10
- Record: found
- Abstract: not found
- Article: not found
Autoimmune Polyendocrine Syndromes
- Record: found
- Abstract: found
- Article: not found
Acute autoimmune-like hepatitis with atypical anti-mitochondrial antibody after mRNA COVID-19 vaccination: A novel clinical entity?
- Record: found
- Abstract: found
- Article: not found