- Record: found
- Abstract: found
- Article: found
Epidemiology of respiratory viral infections in two long-term refugee camps in Kenya, 2007-2010
Read this article at
Abstract
Background
Refugees are at risk for poor outcomes from acute respiratory infections (ARI) because of overcrowding, suboptimal living conditions, and malnutrition. We implemented surveillance for respiratory viruses in Dadaab and Kakuma refugee camps in Kenya to characterize their role in the epidemiology of ARI among refugees.
Methods
From 1 September 2007 through 31 August 2010, we obtained nasopharyngeal (NP) and oropharyngeal (OP) specimens from patients with influenza-like illness (ILI) or severe acute respiratory infections (SARI) and tested them by RT-PCR for adenovirus (AdV), respiratory syncytial virus (RSV), human metapneumovirus (hMPV), parainfluenza viruses (PIV), and influenza A and B viruses. Definitions for ILI and SARI were adapted from those of the World Health Organization. Proportions of cases associated with viral aetiology were calculated by camp and by clinical case definition. In addition, for children < 5 years only, crude estimates of rates due to SARI per 1000 were obtained.
Results
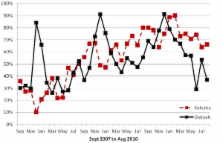
We tested specimens from 1815 ILI and 4449 SARI patients (median age = 1 year). Proportion positive for virus were AdV, 21.7%; RSV, 12.5%; hMPV, 5.7%; PIV, 9.4%; influenza A, 9.7%; and influenza B, 2.6%; 49.8% were positive for at least one virus. The annual rate of SARI hospitalisation for 2007-2010 was 57 per 1000 children per year. Virus-positive hospitalisation rates were 14 for AdV; 9 for RSV; 6 for PIV; 4 for hMPV; 5 for influenza A; and 1 for influenza B. The rate of SARI hospitalisation was highest in children < 1 year old (156 per 1000 child-years). The ratio of rates for children < 1 year and 1 to < 5 years old was 3.7:1 for AdV, 5.5:1 for RSV, 4.4:1 for PIV, 5.1:1 for hMPV, 3.2:1 for influenza A, and 2.2:1 for influenza B. While SARI hospitalisation rates peaked from November to February in Dadaab, no distinct seasonality was observed in Kakuma.
Related collections
Most cited references32
- Record: found
- Abstract: not found
- Article: not found
Respiratory syncytial virus and parainfluenza virus.
- Record: found
- Abstract: found
- Article: not found
Epidemiology and etiology of childhood pneumonia.
- Record: found
- Abstract: found
- Article: not found