- Record: found
- Abstract: found
- Article: found
Laparoscopic diagnosis and treatment of a hydrocele of the canal of Nuck extending in the retroperitoneal space: A case report
Read this article at
Highlights
Abstract
INTRODUCTION
Hydrocele of the canal of Nuck is a rarely encountered entity. We report a case underwent laparoscopic totally extraperitoneal (TEP) treatment for a hydrocele of the canal of Nuck extending in the extraperitoneal space mainly.
PRESENTATION OF CASE
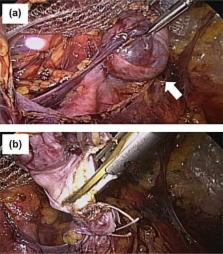
A 37-year-old woman complained of painless and reducible swelling in her left groin, and referred to our hospital for surgical management against left inguinal hernia with the incarcerated ovary. Ultrasonography and MR images revealed a cystic mass in the retroperitoneal space, and we diagnosed as an unusual type of hydrocele of the canal of Nuck. The patient was scheduled for laparoscopic treatment. Laparoscopic findings on pneumoperitoneum showed an extraperitoneal cystic tumor with no contact with the left ovary. The fascia and peritoneum of the port site were closed, and then an extraperitoneal space was created. The cystic tumor with the round ligament of the uterus was dissected and resected by the TEP technique. The extended deep inguinal ring was repaired with polypropylene mesh. Postoperative course was uneventful.
DISCUSSION
Hydrocele of the canal of Nuck in the adult female is a rare condition. The accurate diagnosis of an inguinal hydrocele in a female is seldom made. Laparoscopic examination provides surgeons with information of inguinal swelling accompanied with retroperitoneal cyst, and consecutive treatment by laparoscopic technique, especially TEP, is useful in regard to minimal damage of the peritoneum.
Related collections
Most cited references13
- Record: found
- Abstract: found
- Article: not found
Comparison of conventional anterior surgery and laparoscopic surgery for inguinal-hernia repair.
- Record: found
- Abstract: found
- Article: not found
Imaging of groin masses: inguinal anatomy and pathologic conditions revisited.
- Record: found
- Abstract: found
- Article: not found