Abbreviations: CAD, coronary artery disease; ICC, intraclass correlation coefficient; FMD, flow mediated dilation; PAV, peripheral arterial volume.
Introduction
Coronary artery disease (CAD) has several significant risk factors, among which endothelial dysfunction is critical in the development of atherosclerosis and cardiovascular events [1]. A growing need exists for more convenient and accurate, non-invasive tools to evaluate endothelial function. One commonly used approach for identifying patients at risk of cardiovascular issues is flow-mediated dilation (FMD). However, despite being considered the gold standard in non-invasive testing, FMD has limitations in its reproducibility [2].
FMD relies on assessing changes in arterial diameter [3]. The reproducibility of FMD may vary with differences in detection techniques, measurement locations, and changes in arteries’ ability to dilate with arterial hardening. Recent developments in fingertip non-invasive detection techniques have emerged as a promising alternative to overcome the limitations of high-resolution ultrasound assessments of brachial artery FMD. One such technique is peripheral arterial volume (PAV) [4]. PAV is based on a similar principle to that of FMD, but it uses a different approach from traditional ultrasound methods to assess vascular endothelial function. In PAV a photo-plethysmographic fingertip probe is used to record pulsatile hemoglobin flow, measuring changes in digital arterial volume by using light-emitting diodes (940 nm) and a light-sensitive sensor to evaluate hemoglobin absorbance. The PAV value is calculated according to the difference in digital artery hemoglobin flow before and after occlusion of an upper limb. Notably, PAV minimizes the effects of local venous dilation, and its fingertip probe can be reused multiple times, thus aiding in reproducibility in individuals with coronary heart disease and the general population. Despite many recent studies on PAV, data on the reproducibility of PAV measurements remain limited. Therefore, the purpose of this study was to evaluate PAV reproducibility in a real clinical setting.
Methods
Study Participants
A total of 152 patients presenting with chest pain and admitted to our hospital were included in this study. Their ages ranged from 31 to 80 years. The exclusion criteria were acute coronary syndrome; cardiac insufficiency; persistent atrial fibrillation; severe valvular heart disease; Raynaud’s phenomenon; chronic respiratory, endocrine, or renal conditions; or participation in another clinical trial. The study protocol adhered to the ethical principles outlined in the Declaration of Helsinki and was approved by the ethical review board of the China-Japan Union Hospital of Jilin University. The study was also registered with the Chinese Clinical Trial Registry (ChiCTR-DDD-17011214). All patients provided written informed consent.
Study Design
The study was conducted at the China-Japan Union Hospital of Jilin University Follow-up Center for Cardiology. The PAV technique was used to assess endothelial function in all patients. Although similar in theory to peripheral arterial tonometry (PAT), the PAV technique records hemoglobin flow before and after occlusion of brachial blood flow, as detected by photo-plethysmographic probes. Changes in PAV are reflected in monitoring of pulsatile hemoglobin flow. Before the testing days, patients were instructed to abstain from consuming food, cigarettes, coffee, or tea for at least 12 hours. If there is any eating, smoking, coffee or tea during the process, we will require the subjects to undergo testing the next day. The time interval between two tests should exceed at least 2 hours to avoid the congestion effect left by the previous measurement affecting the results of the next measurement. The subject should rest in a quiet environment for at least 5 minutes before each test, and the ambient temperature should be maintained between 21 and 25 °C. They were also advised to avoid medications that could affect vascular activity, such as nitroglycerin. Clinical participants with chest pain were selected for the study. Patients with acute coronary syndrome; cardiac insufficiency; atrial fibrillation; severe valvular heart disease; Raynaud’s disease; or chronic respiratory, endocrine, or kidney diseases were excluded.
The data collection process involved recording 2-minute baseline amplitude data, inflating the cuff to 180 mmHg, maintaining the occlusion for 3 minutes, and deflating the cuff. Subsequently, 2-minute hyperemia reactive data were recorded. The final PAV was calculated by comparison among the data before and after pressurization, as well as the baseline amplitude data. To establish PAV reproducibility, we collected two measurements under the same conditions on the same day in each patient. Medical baseline data for all enrolled patients were obtained from the inpatient system. The results of the two measurements and patient characteristics, including age, sex, weight, BMI, systolic pressure, and diastolic pressure, are expressed as mean ± standard deviation. Additionally, patients were divided into subgroups by age (with a cutoff of 60 years), sex, and BMI (with a cutoff of 28 kg/m2), and differences among subgroups were analyzed to assess PAV reproducibility.
Evaluation of Peripheral Arterial Volume
PAV measurements were conducted by a single examiner, and two assessments were performed by the same examiner in each participant. Participants were instructed to lie flat on a bed; place the cuff on the left arm at 2 cm above the elbow joint; and attach the PAV probes to the fingertips of both index fingers. The PAV device contained an optical plethysmograph for detecting changes in the quantity of pulsating hemoglobin under uniform pressure, which was applied to the surface of the finger. The PAV measurement process involved inflating the cuff to a pressure 60 mmHg above systolic pressure, thus resulting in a 3-minute occlusion of blood flow on the pressurized side. After occlusion, the cuff was rapidly deflated, thereby inducing reactive congestion, and the PAV signal was recorded from both fingertips. An additional 2 minutes of measurement was performed on the non-pressurized fingertip as a control. The PAV value was automatically calculated by the instrument’s terminal.
Statistical Analysis
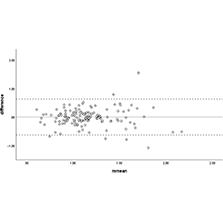
PAV reproducibility was assessed in terms of reliability and consistency [5]. The intraclass correlation coefficient (ICC) was calculated as SDb/(SDb+SDw), where SDb and SDw represents the standard deviations between and within the two measurements, respectively. An ICC value above 0.6 was considered to indicate good reliability [6]. Bland-Altman analysis and the coefficient of variation (CV) were used to evaluate the relationship between the means and differences in the two measurement results. Subsequently, a 95% confidence interval was calculated to assess PAV consistency. The Bland-Altman method was used to illustrate the relationships of PAV1 and PAV2 differences by plotting the differences between the two repeated measurements against their mean value. To better compare the variability in the two measurements, we calculated the CV as 100 × (standard deviation of the paired differences divided by the overall mean divided by the square root of 2), expressed as a percentage.
ICC values within each subgroup were compared between measurements. Statistical significance was determined with paired t-tests; P-values less than 0.05 were considered significant. All statistical analyses were performed in SPSS 25.
Results
Patient Characteristics
A total of 152 patients (55% male) were included in this study. Table 1 presents the demographic information for the participants, including age, sex, height, weight, BMI, systolic blood pressure, diastolic blood pressure, and heart rate. The mean age was 55.8 years, and the mean ± standard deviation values for height and weight were 164.7 ± 7.2 and 67.9 ± 12.7, respectively. The mean ± standard deviation values for systolic and diastolic blood pressure were 117.5 ± 19.4 and 79.2 ± 17.5, respectively. BMI and heart rate were calculated to be 25.0 ± 4.7 and 73.4 ± 11.3, respectively.
Baseline Patient Characteristics.*
| Variable | n = 152 |
|---|---|
| Age (year) | 55.8 ± 12.3 |
| Male sex (%) | 83(55) |
| Height (cm) | 164.7 ± 7.2 |
| Weight (kg) | 67.9 ± 12.7 |
| Body mass index (kg/m2) | 25.0 ± 4.7 |
| Systolic blood pressure (mmHg) | 117.5 ± 19.4 |
| Diastolic blood pressure (mmHg) | 79.2 ± 17.5 |
| Heart rate (beats per minute) | 73.4 ± 11.3 |
*Values are presented as mean ± SD or number (%).
Relationship between PAV1 and PAV2
To evaluate PAV reproducibility, we considered several factors potentially influenced by endothelial function, such as age, BMI, and sex. On the basis of these characteristics, patients were divided into three subgroups, and the results of the two PAV tests were compared within each subgroup.
No significant differences were observed among subgroups (Table 2). The first and second PAV test results were 1.11 ± 0.27 and 1.16 ± 0.30, respectively (P = 0.09), among men, and 1.21 ± 0.38 and 1.15 ± 0.34, respectively (P = 0.19), among women.
Differences in the Two Repeated PAV Measurements According to Patient Characteristics.
| n | PAV measurement 1 | PAV measurement 2 | Mean of differences | P | ICC | |
|---|---|---|---|---|---|---|
| Total | 152 | 1.15 ± 0.33 | 1.15 ± 0.31 | 0.00 ± 0.32 | 0.99 | 0.66 |
| Men | 83 | 1.11 ± 0.27 | 1.16 ± 0.30 | −0.03 ± 0.27 | 0.09 | 0.72 |
| Women | 69 | 1.21 ± 0.38 | 1.15 ± 0.34 | 0.06 ± 0.38 | 0.19 | 0.63 |
| Age <60 years | 85 | 1.22 ± 0.37 | 1.18 ± 0.36 | 0.04 ± 0.37 | 0.33 | 0.64 |
| Age ≥60 years | 67 | 1.07 ± 0.25 | 1.12 ± 0.24 | −0.05 ± 0.24 | 0.09 | 0.70 |
| BMI <28 kg/m2 | 117 | 1.15 ± 0.34 | 1.15 ± 0.31 | 0.00 ± 0.35 | 0.98 | 0.60 |
| BMI ≥28 kg/m2 | 35 | 1.16 ± 0.32 | 1.16 ± 0.33 | 0.00 ± 0.24 | 0.98 | 0.84 |
Values are presented as mean ± SD or number (%). BMI: body mass index, PAV: peripheral artery volume, ICC: intraclass correlation coefficient, CV: coefficient of variation.
Factors Associated with PAV
Patients were categorized into three subgroups by sex, age, and BMI. We evaluated the reliability of PAV measurements within sex subgroups; the ICC was 0.72 in men and 0.63 in women. Among age subgroups, the ICC was 0.64 in participants <60 years and 0.70 in participants ≥60 years. Similar ICC values were observed among BMI subgroups. The ICC was 0.60 for BMI <28 kg/m2 and 0.84 for BMI ≥28 kg/m2.
Analysis of ICCs in each subgroup revealed no significant differences, thus indicating no apparent correlation of PAV measurements with sex, age, or BMI in this clinical study.
Among sex subgroups, the CV was 23.58% for men and 26.10% for women. Among age subgroups, the CV was 25.88% for those <60 years and 20.56% for those ≥60 years. Among BMI subgroups, the CV was 27.31% for those with a BMI <28 kg/m2 and 23.60% for those with a BMI ≥28 kg/m2.
Reproducibility of PAV
To assess the presence of systematic errors, measurement errors, and the reproducibility trends between measurements, we generated a Bland-Altman plot (Figure 1). In the plot, only four data points were located outside the interval, whereas most data were located within the interval. Analysis of all calculated data indicated that the PAV measurements showed good reliability in this clinical study.

Discussion
Numerous studies have recently demonstrated that non-invasive measurements of endothelial function, such as PAV, can predict cardiovascular events. PAV, a novel technique based on photoplethysmography, shares similarities with FMD. PAV measurement is automatic and operator-independent, and avoids subjective error. Compared with FMD, PAV offers a more convenient non-invasive method for assessing fingertip endothelial function. However, because PAV is a novel technique, its reproducibility has not been extensively studied. Prior research [7] has identified a linear correlation between PAV and FMD in patients with chest pain, and has associated PAV with high-risk factors for coronary heart disease, such as diabetes, hypertension, hyperlipidemia, or a family history of CAD. Another study [4] has demonstrated that combining age-adjusted Framingham risk scores with PAV effectively enhances CAD prediction.
Our study confirmed PAV’s reproducibility in assessing endothelial function in adults (ICC = 0.76, CV = 24.49%). This result is particularly notable in comparison to recent results for PAT in adults (ICC = 0.61, CV = 18.0%) and the ICC range of FMD (0.54 to 0.92) across different groups such as people with differences in race, age, and risk factors for coronary heart disease, etc. [8]. The differences observed in ICC and CV among various detection techniques are not substantial. Furthermore, PAV has not been found to significantly correlate with age, sex, or BMI in the adult population. Thus PAV, as a novel technique for evaluating fingertip endothelial function, has reliable reproducibility. Previous studies have established that sex, BMI, and age can impair endothelial function but do not significantly affect PAV.
Endothelial dysfunction not only is an independent predictor of cardiovascular disease prognosis but also plays a crucial role in the progression of coronary atherosclerosis [9]. Methods for assessing endothelial function are rapidly evolving, and interest in non-invasive detection of vascular endothelial function is growing, because of these methods’ convenience and good reproducibility. Consequently, evaluating the reproducibility of non-invasive methods is valuable.
FMD, considered the “gold standard” for non-invasive assessment of endothelial function [10], has versatile applications. However, it primarily reflects the endothelial function of larger vessels and is responsive to only conventional risk factors. Its primary drawback lies in its limited repeatability, owing to operator-dependent factors, thus leading to potential errors during the measurement process [3]. Recently, fingertip non-invasive detection has emerged as an innovative method for assessing endothelial function and has demonstrated noteworthy potential for predicting cardiovascular events [4].
PAV has advantages such as the ability to exclude distal venous dilation caused by occlusion, and to use probes repeatedly [7]. As described in previous studies, PAV can be used not only to predict coronary heart disease [7] but also to assess its practicality in clinical practice. In this study, to evaluate PAV reproducibility, we collected a sample of endothelial function data from 152 adults with chest pain to evaluate, and found that PAV had good reproducibility. PAV reproducibility is influenced by various factors, including participants and environmental conditions. To minimize systematic errors, we implemented a rigorous experimental protocol and calculated PAV values twice by using precise instruments, to assess the repeatability of PAV in clinical applications among individuals.
To simultaneously evaluate the effects of age, BMI, and sex on PAV reproducibility, we conducted all tests in a consistent environment. Analysis of the degree of dispersion with the Bland-Altman plot demonstrated the favorable consistency of PAV. In comparison to past data on PAT reproducibility, the Bland-Altman plot indicated that PAT results demonstrated good consistency across experiments, despite variations in patient characteristics including sex, age, and BMI. In our sex subgroup analyses of PAV reproducibility, the CV was lower in men than women, in agreement with guidelines indicating that sex is a risk factor for coronary heart disease. In age subgroup analysis, the CV was higher in individuals <60 years of age, thus suggesting a decline in endothelial function with advancing age. When the BMI was ≥28 kg/m2, rather than <28 kg/m2, a relatively lower CV was observed, thereby indicating that obesity contributes to changes in arterial blood flow and further affects endothelial function.
Despite being considered the gold standard for non-invasive testing technology, FMD has a notable drawback arising from its subjective measurement. According to FMD guidelines, a mean difference of 20%–30% is deemed acceptable [5]. However, the data from our PAV study showed a 24.49% difference. Studies have verified that the ICC for PAT in adults is 0.61 [11], and the ICC range of FMD was 0.54 to 0.92 as mentioned earlier, the ICC of PAV was 0.66 in this study, therefore, the reproducibility of PAV also seems reliable [12]. The ICC, reflecting the consistency between two measurements, demonstrated the good reproducibility of PAV in this clinical study in adults, thus highlighting the inherent advantages of this technique. Grounded in PAT theory [13–15], PAV is a reliable fingertip technique for evaluating endothelial function in the adult population. Although few studies have assessed PAV’s repeatability, several findings support its application. First, non-invasive fingertip techniques, beyond assessing endothelial function in coronary heart disease, can also be used to evaluate endothelial function in healthy adult populations, thus supporting the development of non-invasive fingertip detection for endothelial function [15] and screening for coronary heart disease, and timely prediction and evaluation of coronary heart disease [16]. Second, when considering risk factors for coronary heart disease, stratification of test samples, primarily by age, sex, or BMI, indicated no significant differences in PAV reproducibility. In contrast, the repeatability of PAT enables applications in detecting endothelial function not only in patients with coronary heart disease but also in patients with heart failure and hypertension, as indicated by previous studies [17]. Further research is required to evaluate the repeatability of PAV.
PAV, a novel non-invasive fingertip measurement for predicting CAD, has major application prospects for patients with CAD. Of note, the age range of patients included in this study was 31–80 years, and the sample sizes were relatively small; consequently, our PAV reproducibility measurements were relatively limited. To conveniently assess endothelial function in the broader population, expanding the characteristics of the population will be essential for PAV test.
Although limited data are available on the reproducibility and reliability of PAV measurements, evidence suggests that PAV can predict the development of cardiovascular disease and improve prognosis in clinical applications. PAV holds promise as a fingertip technique for assessing endothelial function and evaluating the risk factors for multiple coronary diseases in asymptomatic or subclinical populations.