- Record: found
- Abstract: found
- Article: found
Association of long-term triglyceride-glucose index patterns with the incidence of chronic kidney disease among non-diabetic population: evidence from a functional community cohort
Read this article at
Abstract
Background
The triglyceride-glucose (TyG) index is a reliable surrogate marker of insulin resistance and previous studies have confirmed the association of TyG index with incident chronic kidney disease (CKD). However, the impact of longitudinal patterns of TyG index on CKD risk among non-diabetic population is still unknown. Therefore, this study aimed to investigate the association of longitudinal patterns of TyG index with incident CKD among non-diabetic population.
Methods
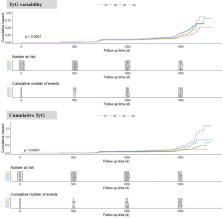
A total of 5484 non-diabetic participants who underwent one health examination per year from 2015 to 2017 were included in this prospective study. TyG index variability and cumulative TyG index were calculated to assess the longitudinal patterns of TyG index. Cox proportional hazard models were performed to estimate the association of TyG index variability or cumulative TyG index with incident CKD.
Results
During a median of 3.82 years follow-up, 879 participants developed CKD. Compared with participants in the lowest quartile, the hazard ratio (HR) and 95% confidence interval (CI) of incident CKD were 1.772 (95% CI: 1.453, 2.162) for the highest TyG index variability quartile and 2.091 (95% CI: 1.646, 2.655) for the highest cumulative TyG index quartile in the fully adjusted models. The best discrimination and reclassification improvement were observed after adding baseline TyG, TyG index variability and cumulative TyG index to the clinical risk model for CKD.
Related collections
Most cited references38
- Record: found
- Abstract: found
- Article: not found
Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization.
- Record: found
- Abstract: found
- Article: not found
The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects.
- Record: found
- Abstract: found
- Article: not found