- Record: found
- Abstract: found
- Article: found
Rapid Transition to Telehealth and the Digital Divide: Implications for Primary Care Access and Equity in a Post‐COVID Era
Read this article at

Abstract
-
Telehealth has many potential advantages during an infectious disease outbreak such as the COVID‐19 pandemic, and the COVID‐19 pandemic has accelerated the shift to telehealth as a prominent care delivery mode.
-
Not all health care providers and patients are equally ready to take part in the telehealth revolution, which raises concerns for health equity during and after the COVID‐19 pandemic.
-
Without proactive efforts to address both patient‐ and provider‐related digital barriers associated with socioeconomic status, the wide‐scale implementation of telehealth amid COVID‐19 may reinforce disparities in health access in already marginalized and underserved communities.
-
To ensure greater telehealth equity, policy changes should address barriers faced overwhelmingly by marginalized patient populations and those who serve them.
Context
The COVID‐19 pandemic has catalyzed fundamental shifts across the US health care delivery system, including a rapid transition to telehealth. Telehealth has many potential advantages, including maintaining critical access to care while keeping both patients and providers safe from unnecessary exposure to the coronavirus. However, not all health care providers and patients are equally ready to take part in this digital revolution, which raises concerns for health equity during and after the COVID‐19 pandemic.
Methods
The study analyzed data about small primary care practices’ telehealth use and barriers to telehealth use collected from rapid‐response surveys administered by the New York City Department of Health and Mental Hygiene's Bureau of Equitable Health Systems and New York University from mid‐April through mid‐June 2020 as part of the city's efforts to understand how primary care practices were responding to the COVID‐19 pandemic following New York State's stay‐at‐home order on March 22. We focused on small primary care practices because they represent 40% of primary care providers and are disproportionately located in low‐income, minority or immigrant areas that were more severely impacted by COVID‐19. To examine whether telehealth use and barriers differed based on the socioeconomic characteristics of the communities served by these practices, we used the Centers for Disease Control and Prevention Social Vulnerability Index (SVI) to stratify respondents as being in high‐SVI or low‐SVI areas. We then characterized respondents’ telehealth use and barriers to adoption by using means and proportions with 95% confidence intervals. In addition to a primary analysis using pooled data across the five waves of the survey, we performed sensitivity analyses using data from respondents who only took one survey, first wave only, and the last two waves only.
Findings
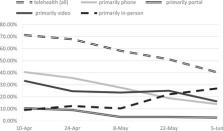
While all providers rapidly shifted to telehealth, there were differences based on community characteristics in both the primary mode of telehealth used and the types of barriers experienced by providers. Providers in high‐SVI areas were almost twice as likely as providers in low‐SVI areas to use telephones as their primary telehealth modality (41.7% vs 23.8%; P <.001). The opposite was true for video, which was used as the primary telehealth modality by 18.7% of providers in high‐SVI areas and 33.7% of providers in low‐SVI areas ( P <0.001). Providers in high‐SVI areas also faced more patient‐related barriers and fewer provider‐related barriers than those in low‐SVI areas.
Conclusions
Between April and June 2020, telehealth became a prominent mode of primary care delivery in New York City. However, the transition to telehealth did not unfold in the same manner across communities. To ensure greater telehealth equity, policy changes should address barriers faced overwhelmingly by marginalized patient populations and those who serve them.
Related collections
Most cited references45
- Record: found
- Abstract: not found
- Article: not found
Virtually Perfect? Telemedicine for Covid-19
- Record: found
- Abstract: found
- Article: found
Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19)

- Record: found
- Abstract: found
- Article: found