- Record: found
- Abstract: found
- Article: found
Spontaneous Pneumomediastinum, Pneumopericardium, and Pneumothorax with Respiratory Failure in a Patient with AIDS and Pneumocystis jirovecii Pneumonia
Read this article at
Abstract
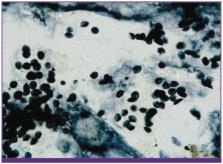
Spontaneous pneumothorax occurs in up to 35% of patients with Pneumocystis jirovecii pneumonia. However, spontaneous pneumomediastinum and pneumopericardium are uncommon complications in patients infected with human immunodeficiency virus, with no reported incidence rates, even among patients with acquired immunodeficiency syndrome (AIDS) and P. jirovecii pneumonia. We report a case of spontaneous pneumomediastinum, pneumopericardium, and pneumothorax with respiratory failure during treatment of P. jirovecii pneumonia in a patient with AIDS; the P. jirovecii infection was confirmed by performing methenamine silver staining of bronchoalveolar lavage specimens. This case suggests that spontaneous pneumomediastinum and pneumopericardium should be considered in patients with AIDS and P. jirovecii pneumonia.
Related collections
Most cited references19
- Record: found
- Abstract: found
- Article: found
A New Name for Pneumocystis from Humans and New Perspectives on the Host-Pathogen Relationship
- Record: found
- Abstract: found
- Article: not found