- Record: found
- Abstract: found
- Article: found
Integrated disease prevention campaigns: assessing country opportunity for implementation via an index approach
Read this article at
Abstract
Objectives
To help stakeholders identify and prioritise countries with the best opportunities for implementation of an integrated prevention campaign (IPC) focused on diarrhoea, malaria and HIV prevention.
Design
Cross-sectional analysis of country-specific epidemiological data using an index tool developed for this purpose.
Setting
We calculated the total disability-adjusted life years (DALYs) attributed to diarrhoea, malaria and HIV for 214 World Bank economies. Criteria for inclusion were: low-income and middle-income countries, and total annual DALY burden in the top tertile (≥87 000 DALYs). 70 countries met inclusion criteria and were included in our opportunity analysis.
Outcome measures
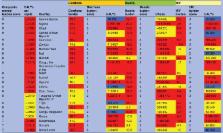
We synthesised data on 10 indicators related to the potential reduction in burden and new coverage achievable by an IPC. We scored and ranked countries based on three summary opportunity metrics: DALYs per capita across the diseases, a composite score of tertile rankings of burden for each disease, and a score combining burden and intervention opportunity.
Results
We estimated the total annual global burden attributable to diarrhoea, malaria and HIV at 135 million DALYs. All of the countries with the highest opportunity for implementation of a diarrhoea, malaria and HIV IPC are in sub-Saharan Africa, regardless of opportunity metric used. Although the overall rank order changes, 16 countries rank among the top 23 highest opportunity countries for all three metrics.
Related collections
Most cited references17
- Record: found
- Abstract: found
- Article: not found
Global, regional, and national causes of child mortality in 2008: a systematic analysis

- Record: found
- Abstract: found
- Article: found
Diarrhea incidence in low- and middle-income countries in 1990 and 2010: a systematic review
- Record: found
- Abstract: found
- Article: not found