- Record: found
- Abstract: found
- Article: found
Factors Associated with Early Mortality in Critically Ill Patients Following the Initiation of Continuous Renal Replacement Therapy
Read this article at
Abstract
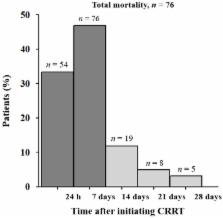
Continuous renal replacement therapy (CRRT) is an important modality to support critically ill patients, and the need for CRRT treatment has been increasing. However, CRRT management is costly, and the associated resources are limited. Thus, it remains challenging to identify patients that are likely to have a poor outcome, despite active treatment with CRRT. We sought to elucidate the factors associated with early mortality after CRRT initiation. We analyzed 240 patients who initiated CRRT at an academic medical center between September 2016 and January 2018. We compared baseline characteristics between patients who died within seven days of initiating CRRT (early mortality), and those that survived more than seven days beyond the initiation of CRRT. Of the patients assessed, 130 (54.2%) died within seven days of CRRT initiation. Multivariate logistic regression models revealed that low mean arterial pressure, low arterial pH, and high Sequential Organ Failure Assessment score before CRRT initiation were significantly associated with increased early mortality in patients requiring CRRT. In conclusion, the mortality within seven days following CRRT initiation was very high in this study. We identified several factors that are associated with early mortality in patients undergoing CRRT, which may be useful in predicting early outcomes, despite active treatment with CRRT.
Related collections
Most cited references39
- Record: found
- Abstract: found
- Article: not found
Continuous renal replacement therapy: a worldwide practice survey. The beginning and ending supportive therapy for the kidney (B.E.S.T. kidney) investigators.
- Record: found
- Abstract: found
- Article: not found
Epidemiology and outcomes of acute renal failure in hospitalized patients: a national survey.

- Record: found
- Abstract: found
- Article: found